How to Create Psychiatric SOAP Notes [+ Free Template]
Unlike specialties where objective tests can tell the whole story, psychiatry is all about nuance.
Every word choice, emotional response, and micro-expression plays its role in your diagnosis and treatment.
But when you’re splitting attention between patients and paperwork, it's easy to miss critical risk markers that could impact patient progress.
Psychiatric SOAP notes can change things.
These notes offer a clear structure to organize information efficiently — without sacrificing clinical detail or adding hours to your day.
Let's explore how psychiatric SOAP notes can help you be fully present with patients and get rid of pajama time.
What purpose does the SOAP note serve?
SOAP notes in psychiatry give clinicians an organized and actionable format to document patient interactions and observations
You know it: even the most subtle changes in mood, thought patterns, and behavior could indicate significant developments.
With properly documented SOAP notes, clinicians can deliver better care and improve patient outcomes.
Besides tracking patient progress, these SOAP notes help psychiatrists:
- Create billing paperwork for insurance providers
- Support diagnostic decisions with clear evidence
- Ensure continuity of care without losing info
More importantly, psychiatric SOAP notes can make charting faster, easier, and more efficient.
So, you don’t have to end your day drowning in paperwork and trying to reconstruct conversations from memory.
If you’re wondering how SOAP notes differ from psychotherapy notes, let’s look at the key differences.
SOAP notes vs. Psychotherapy notes: How do they differ
Psychiatrists prepare both SOAP notes and psychotherapy notes (also called progress notes). However, these two charts have entirely different use cases.
SOAP notes are added to a patient’s official medical record.
They focus on clinical observations, diagnostic information, and treatment plans that directly justify medical necessity. These notes are also used for billing purposes.
Psychotherapy notes are completely private to a clinician and not added to the official record.
These notes capture a clinician’s subjective thoughts, observations, and hypotheses during a therapy session. They help clinicians process all the information and make diagnostic decisions.
Here are some key points of difference between SOAP notes and psychotherapy notes:
Category SOAP Notes Psychotherapy Notes Purpose Communicate medical information to other providers and justify billing Support the therapist's own clinical thinking and treatment planning Focus Document symptoms, diagnoses, medications, and treatment plans Contain session content, therapist impressions, and analysis useful for clinical reasoning but not necessary for others Legal Requirements Must meet documentation standards for reimbursement and medical necessity Optional but valuable for clinical development Time Investment Need to be concise yet complete Can be as detailed or sparse as helps your clinical process Accessibility Can be requested by patients, insurance companies, and other providers Receive special privacy protections under HIPAA and generally can't be accessed without specific authorization
Knowing this difference means you can be more compliant and not scramble at the last minute to redact sensitive information from your SOAP notes.
📋 Check out this resource: Free Progress Notes Templates and Sanity-Saving Hacks
Psychiatric SOAP note template (and how it works)
Wondering how to prepare these structured notes for your psychiatry practice?
Here’s our psychiatric SOAP note template to make things easier for you.
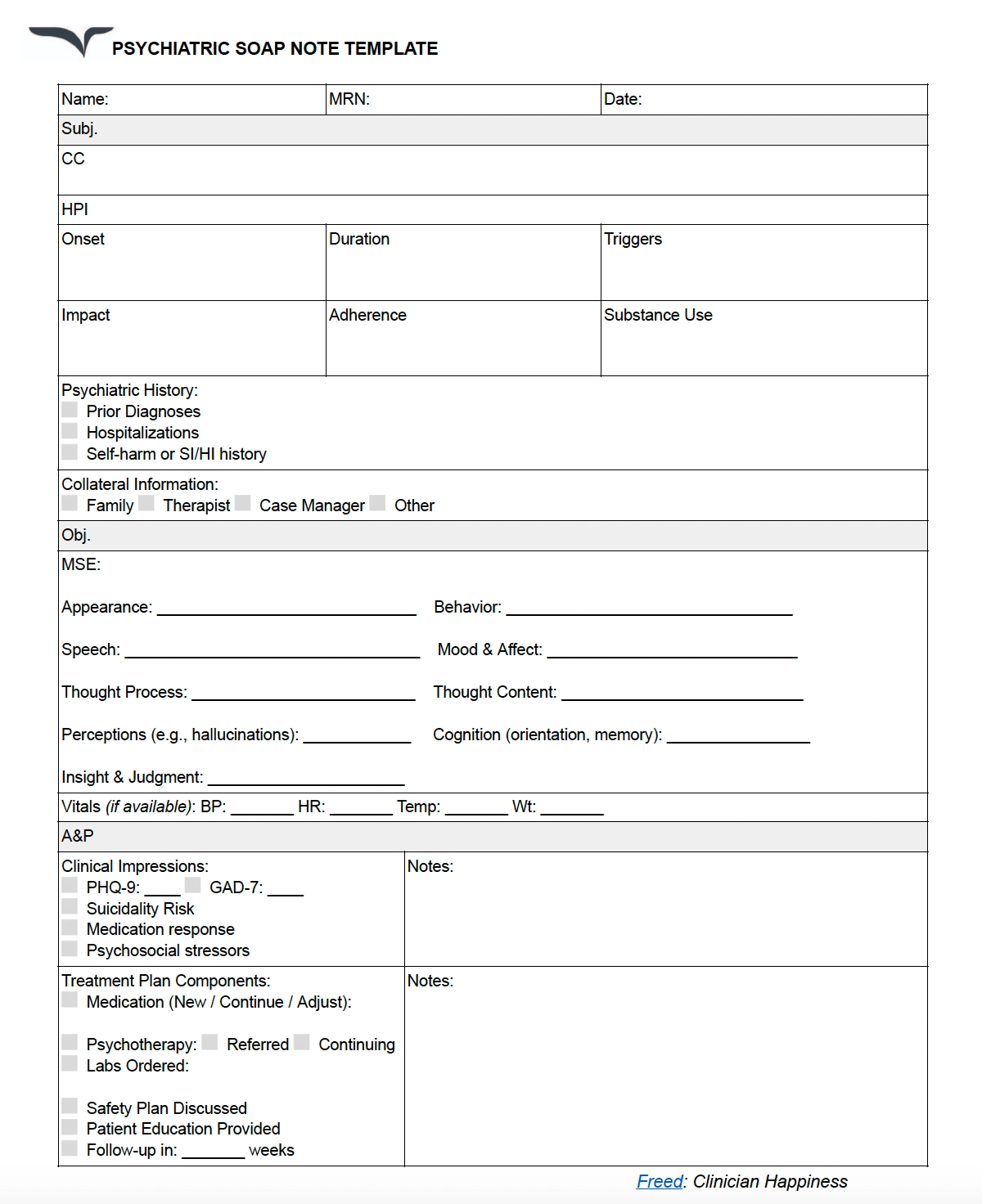
Let’s look at an example to see how this template works.
Andy is a 30-year-old sales executive feeling overwhelmed with his new job. Here are the SOAP notes from his first psychiatry session:
Subjective: The patient, a 30-year-old male, reports “feeling overwhelmed” for the last three months. Symptoms include persistent low mood, concentration difficulties, sleep onset insomnia, early waking, 7lb weight loss, and irritability. He describes a feeling of constant pressure at his job, stating, “I have to push myself to work extra hours every week.” Self-management with exercise and meditation showed minimal benefit. He has a family history of depression.
Objective: The patient appears well-groomed but tired. Mood "stressed and down" with constricted affect. Logical thought process, no thought abnormalities. Alert and oriented with mild concentration impairment. Good insight and intact judgment.
Vitals stable: BP 128/82, HR 88
Assessment:
- Major Depressive Disorder, moderate (F32.1)
- Generalized Anxiety Disorder (F41.1)
- R/O Adjustment Disorder with mixed anxiety/depression
- Occupational problem
Plan:
- Medication: Sertraline 50mg daily x1 week, then 100mg; Lorazepam 0.5mg PRN (max 6)
- Sleep hygiene and exercise recommendations
- Follow-up in 2 weeks with rating scales
- Basic labs to rule out medical causes
- Safety plan and resources provided
You can also prepare a treatment plan for this patient to discuss how you want to improve his condition.
Here’s a summarized treatment plan for psychiatry:
Goals and objectives
Long-term goal 1: Reduce depressive symptoms to a minimal or mild range (PHQ-9 < 10)
Objective 1: Increase daily activities and social engagement
Intervention(s):
- Behavioral activation
- Medication management with sertraline
- Weekly CBT therapy sessions
Duration/Frequency: Daily activity scheduling, weekly therapy for 3 months
Objective 2: Improve sleep quality and duration
Intervention(s):
- Sleep hygiene education
- Medication management
- Cognitive strategies for nighttime rumination
Duration/Frequency: Daily sleep log monitoring for 1 month
Long-term goal 2: Reduce anxiety symptoms to mild range (GAD-7 < 10)
Objective 1: Develop effective anxiety management skills
Intervention(s):
- Progressive muscle relaxation training
- Mindfulness exercises
- Cognitive restructuring of anxious thoughts
Duration/Frequency: Daily practice for 4 weeks
Objective 2: Reduce physiological symptoms of anxiety
Intervention(s):
- Diaphragmatic breathing
- Medication management
- Regular physical exercise
Duration/Frequency: 3x daily breathing exercises, 30 min exercise 5x/week
How to write SOAP notes in psychiatry
Your psychiatry practice moves at lightning speed. But your memory can't keep up.
That’s why you need SOAP notes to track every detail in your patient conversations without missing a beat. Here’s how to prepare these notes as a psychiatrist.
Document medical necessity with precision
Insurance companies require clear evidence that your services are medically necessary.
Vague documentation = Claim denials.
So, start by including patient quotes that show the impact of their current symptoms.
You can document failed attempts at self-management to highlight the need for clinical intervention. Besides noting symptoms, connect them to functional disabilities in daily life, like work and relationships.
Use descriptive language to capture the impact of their condition. For medication management visits, discuss how current symptoms require continued clinical oversight.
Here’s an example
The patient's anxiety symptoms (persistent worry, insomnia, difficulty concentrating) have resulted in two missed project deadlines at work and significant relationship strain. He describes it as “a complete lack of motivation to focus on anything.” Self-directed breathing exercises provided minimal relief. Current management and weekly CBT are medically necessary to prevent further deterioration.
Support your diagnosis with DSM-5 criteria
Your documentation should share the rationale behind your clinical decisions and justify your treatment approach. Think of it as your audit trail showing diagnostic reasoning.
Here’s how you can support your diagnosis with criteria:
- Specify exact DSM criteria: Document exactly which criteria support your diagnosis to create more transparency. For example:“Patient meets 7/9 DSM-5 criteria for MDD including depressed mood, anhedonia, sleep disturbance, feelings of worthlessness, and diminished concentration.”
- Document negative findings: Rule out similar conditions to strengthen your arguments. For example: “No history of manic episodes to suggest bipolar disorder.”
- Add diagnostic specifiers: DSM-5 specifiers make your documentation more accurate and guide treatment planning. For example: “MDD, moderate, with anxious distress. PTSD with delayed expression.”
- Note differential diagnoses: When you don’t have a clear diagnosis, document all possible diagnoses you’re considering to arrive at the final one. For example: “Differential diagnoses include Generalized Anxiety Disorder vs. Adjustment Disorder with anxiety. Will monitor for the persistence of symptoms beyond 6 months to clarify the diagnosis.”
You need these DSM-5 criteria to create a strong line of defense if and when an audit happens.
Quantify symptoms and progress
Objective measures are equally important to clearly record symptom severity and treatment response. These measures also demonstrate clinical improvement over time.
Use standardized rating scales consistently across visits. You can note down both numerical scores and their clinical interpretation.
At the start of treatment, you can set targets for improvement for specific parameters and track progress. Remember to establish a baseline to monitor the progress trajectory.
Here’s an example
PHQ-9 score decreased from 21 to 16, indicating modest improvement but continued moderately severe depression. Greatest improvement noted in sleep (score changed from 3 to 1), while concentration difficulties remain unchanged (score 3). Patient reports returning to work part-time this week, representing functional improvement from baseline.
Document risk assessments thoroughly
Every psychiatric SOAP note should include an assessment of risk factors like suicidal/homicidal intent.
You need this explicit screening for suicidal and homicidal ideation to establish appropriate standards of care. Assess and document both risk factors and protective factors that inform your clinical judgment.
Like with every other aspect, note any changes in risk status compared to previous visits. Then, discuss your clinical decision-making for the kind of intervention required.
It’s important to state your rationale for possible interventions considered but not implemented.
Here’s an example
Suicide risk assessment completed. Patient acknowledges passive thoughts of 'not wanting to be here anymore' but denies active suicidal ideation, plan, or intent. No history of attempts.
Protective factors include strong connection to children, religious beliefs prohibiting suicide, willingness to engage in treatment, and agreement to a safety plan. Safety plan reviewed and updated today; patient contracted to call crisis line if thoughts worsen before next appointment.
Justify medication decisions explicitly
Document your rationale for starting, continuing, adjusting, or discontinuing medications.
This will support the necessity for each medication and reduce liability.
Share your reasoning for prescribing each medication, dose adjustment, or discontinuation. You have to track the benefits and side effects of each medicine. Mention patient-reported adherence and any barriers to adherence they experience.
You can also add any medication education you’ve offered to help patients understand their role.
Here’s an example
Increasing escitalopram from 10mg to 15mg daily due to partial response (GAD-7 decreased from 18 to 12) with good tolerability after 4 weeks. Patient reports improved ability to fall asleep but continued daily anxiety symptoms interfering with work performance. Discussed potential side effects of increased dose, including possible QT prolongation; assessed benefits to outweigh risks. Patient agreeable to increase.
Addressing concerns about SOAP notes in psychiatry
I get it: You likely have some questions and concerns about implementing psychiatric SOAP notes.
Let me answer some of the most common concerns about these notes.
Concern 1: Is my patient information safe with detailed SOAP notes?
Your patient information is always protected.
While SOAP notes are more accessible than psychotherapy notes, they’re still governed by HIPAA regulations. That means only healthcare providers directly working with a patient can access these notes. You can also use a secure EHR platform to protect your notes further.
Concern 2: Will SOAP notes limit my ability to document nuanced psychiatric observations?
The SOAP note format gives you the space to capture every nuance in a patient conversation.
You can use the Assessment section to document your observations and clinical interpretation. This is your space to note observations around behavior patterns, responses to interventions, and other details.
Here’s the best part: You can customize our psychiatric SOAP notes template to match your style and maintain the depth of your observations.
Concern 3: Do SOAP notes create more documentation burden?
Done well, SOAP notes can actually reduce documentation time.
When you use a consistent template, it’s easier to organize all the insights and observations into the right sections. This way, you can document during or immediately after a session and prevent backlog.
Besides, an AI medical scribe like Freed can do all the heavy lifting on your behalf to prepare in-depth psychiatry SOAP notes.
Simply record your patient conversations with Freed, and it’ll generate detailed notes in the SOAP format. Edit them, save them to your EHR, or print them out—it’s completely up to you. Freed also deletes conversation recordings after 30 days to maintain confidentiality.
Concern 4: What should I include and exclude in my psychiatric SOAP notes?
Effective SOAP notes for psychiatry balance comprehensives with patient privacy. Let’s discuss what to include and exclude in these notes.
Include
- Relevant symptoms, behaviors, and statements that support the diagnosis
- Risk assessments, including suicidal and homicidal ideation screening
- Medication responses, side effects, and adherence information
- Objective observations of mental status and functioning
- Assessment and treatment plan with follow-ups
Exclude
- Details that could stigmatize the patient if the record were accessed
- Personal reactions to the patient that aren't clinically relevant
- Subjective judgments about character or personality
- Speculative diagnoses without supporting evidence
- Irrelevant personal details about the patient's life
Be more present for your patients and for yourself with Freed
Documentation is a double-edged sword for psychiatrists.
It’s essential for tracking patient progress and maintaining compliance. Yet, it can consume all your attention and time needed for meaningful therapeutic connection.
This impossible choice — fully engaging with patients or spending evenings on paperwork — doesn't have to be yours anymore.
Freed can be the ultimate blessing for psychiatrists.
The AI SOAP note Generator works in the background while you give patients your undivided attention. And your SOAP notes are ready before the patient even exits your clinic.
Try Freed to see how it can speed up documentation.
Your future self (and your patients) will thank you.
Table of Contents
Unlike specialties where objective tests can tell the whole story, psychiatry is all about nuance.
Every word choice, emotional response, and micro-expression plays its role in your diagnosis and treatment.
But when you’re splitting attention between patients and paperwork, it's easy to miss critical risk markers that could impact patient progress.
Psychiatric SOAP notes can change things.
These notes offer a clear structure to organize information efficiently — without sacrificing clinical detail or adding hours to your day.
Let's explore how psychiatric SOAP notes can help you be fully present with patients and get rid of pajama time.
What purpose does the SOAP note serve?
SOAP notes in psychiatry give clinicians an organized and actionable format to document patient interactions and observations
You know it: even the most subtle changes in mood, thought patterns, and behavior could indicate significant developments.
With properly documented SOAP notes, clinicians can deliver better care and improve patient outcomes.
Besides tracking patient progress, these SOAP notes help psychiatrists:
- Create billing paperwork for insurance providers
- Support diagnostic decisions with clear evidence
- Ensure continuity of care without losing info
More importantly, psychiatric SOAP notes can make charting faster, easier, and more efficient.
So, you don’t have to end your day drowning in paperwork and trying to reconstruct conversations from memory.
If you’re wondering how SOAP notes differ from psychotherapy notes, let’s look at the key differences.
SOAP notes vs. Psychotherapy notes: How do they differ
Psychiatrists prepare both SOAP notes and psychotherapy notes (also called progress notes). However, these two charts have entirely different use cases.
SOAP notes are added to a patient’s official medical record.
They focus on clinical observations, diagnostic information, and treatment plans that directly justify medical necessity. These notes are also used for billing purposes.
Psychotherapy notes are completely private to a clinician and not added to the official record.
These notes capture a clinician’s subjective thoughts, observations, and hypotheses during a therapy session. They help clinicians process all the information and make diagnostic decisions.
Here are some key points of difference between SOAP notes and psychotherapy notes:
Category SOAP Notes Psychotherapy Notes Purpose Communicate medical information to other providers and justify billing Support the therapist's own clinical thinking and treatment planning Focus Document symptoms, diagnoses, medications, and treatment plans Contain session content, therapist impressions, and analysis useful for clinical reasoning but not necessary for others Legal Requirements Must meet documentation standards for reimbursement and medical necessity Optional but valuable for clinical development Time Investment Need to be concise yet complete Can be as detailed or sparse as helps your clinical process Accessibility Can be requested by patients, insurance companies, and other providers Receive special privacy protections under HIPAA and generally can't be accessed without specific authorization
Knowing this difference means you can be more compliant and not scramble at the last minute to redact sensitive information from your SOAP notes.
📋 Check out this resource: Free Progress Notes Templates and Sanity-Saving Hacks
Psychiatric SOAP note template (and how it works)
Wondering how to prepare these structured notes for your psychiatry practice?
Here’s our psychiatric SOAP note template to make things easier for you.
Let’s look at an example to see how this template works.
Andy is a 30-year-old sales executive feeling overwhelmed with his new job. Here are the SOAP notes from his first psychiatry session:
Subjective: The patient, a 30-year-old male, reports “feeling overwhelmed” for the last three months. Symptoms include persistent low mood, concentration difficulties, sleep onset insomnia, early waking, 7lb weight loss, and irritability. He describes a feeling of constant pressure at his job, stating, “I have to push myself to work extra hours every week.” Self-management with exercise and meditation showed minimal benefit. He has a family history of depression.
Objective: The patient appears well-groomed but tired. Mood "stressed and down" with constricted affect. Logical thought process, no thought abnormalities. Alert and oriented with mild concentration impairment. Good insight and intact judgment.
Vitals stable: BP 128/82, HR 88
Assessment:
- Major Depressive Disorder, moderate (F32.1)
- Generalized Anxiety Disorder (F41.1)
- R/O Adjustment Disorder with mixed anxiety/depression
- Occupational problem
Plan:
- Medication: Sertraline 50mg daily x1 week, then 100mg; Lorazepam 0.5mg PRN (max 6)
- Sleep hygiene and exercise recommendations
- Follow-up in 2 weeks with rating scales
- Basic labs to rule out medical causes
- Safety plan and resources provided
You can also prepare a treatment plan for this patient to discuss how you want to improve his condition.
Here’s a summarized treatment plan for psychiatry:
Goals and objectives
Long-term goal 1: Reduce depressive symptoms to a minimal or mild range (PHQ-9 < 10)
Objective 1: Increase daily activities and social engagement
Intervention(s):
- Behavioral activation
- Medication management with sertraline
- Weekly CBT therapy sessions
Duration/Frequency: Daily activity scheduling, weekly therapy for 3 months
Objective 2: Improve sleep quality and duration
Intervention(s):
- Sleep hygiene education
- Medication management
- Cognitive strategies for nighttime rumination
Duration/Frequency: Daily sleep log monitoring for 1 month
Long-term goal 2: Reduce anxiety symptoms to mild range (GAD-7 < 10)
Objective 1: Develop effective anxiety management skills
Intervention(s):
- Progressive muscle relaxation training
- Mindfulness exercises
- Cognitive restructuring of anxious thoughts
Duration/Frequency: Daily practice for 4 weeks
Objective 2: Reduce physiological symptoms of anxiety
Intervention(s):
- Diaphragmatic breathing
- Medication management
- Regular physical exercise
Duration/Frequency: 3x daily breathing exercises, 30 min exercise 5x/week
How to write SOAP notes in psychiatry
Your psychiatry practice moves at lightning speed. But your memory can't keep up.
That’s why you need SOAP notes to track every detail in your patient conversations without missing a beat. Here’s how to prepare these notes as a psychiatrist.
Document medical necessity with precision
Insurance companies require clear evidence that your services are medically necessary.
Vague documentation = Claim denials.
So, start by including patient quotes that show the impact of their current symptoms.
You can document failed attempts at self-management to highlight the need for clinical intervention. Besides noting symptoms, connect them to functional disabilities in daily life, like work and relationships.
Use descriptive language to capture the impact of their condition. For medication management visits, discuss how current symptoms require continued clinical oversight.
Here’s an example
The patient's anxiety symptoms (persistent worry, insomnia, difficulty concentrating) have resulted in two missed project deadlines at work and significant relationship strain. He describes it as “a complete lack of motivation to focus on anything.” Self-directed breathing exercises provided minimal relief. Current management and weekly CBT are medically necessary to prevent further deterioration.
Support your diagnosis with DSM-5 criteria
Your documentation should share the rationale behind your clinical decisions and justify your treatment approach. Think of it as your audit trail showing diagnostic reasoning.
Here’s how you can support your diagnosis with criteria:
- Specify exact DSM criteria: Document exactly which criteria support your diagnosis to create more transparency. For example:“Patient meets 7/9 DSM-5 criteria for MDD including depressed mood, anhedonia, sleep disturbance, feelings of worthlessness, and diminished concentration.”
- Document negative findings: Rule out similar conditions to strengthen your arguments. For example: “No history of manic episodes to suggest bipolar disorder.”
- Add diagnostic specifiers: DSM-5 specifiers make your documentation more accurate and guide treatment planning. For example: “MDD, moderate, with anxious distress. PTSD with delayed expression.”
- Note differential diagnoses: When you don’t have a clear diagnosis, document all possible diagnoses you’re considering to arrive at the final one. For example: “Differential diagnoses include Generalized Anxiety Disorder vs. Adjustment Disorder with anxiety. Will monitor for the persistence of symptoms beyond 6 months to clarify the diagnosis.”
You need these DSM-5 criteria to create a strong line of defense if and when an audit happens.
Quantify symptoms and progress
Objective measures are equally important to clearly record symptom severity and treatment response. These measures also demonstrate clinical improvement over time.
Use standardized rating scales consistently across visits. You can note down both numerical scores and their clinical interpretation.
At the start of treatment, you can set targets for improvement for specific parameters and track progress. Remember to establish a baseline to monitor the progress trajectory.
Here’s an example
PHQ-9 score decreased from 21 to 16, indicating modest improvement but continued moderately severe depression. Greatest improvement noted in sleep (score changed from 3 to 1), while concentration difficulties remain unchanged (score 3). Patient reports returning to work part-time this week, representing functional improvement from baseline.
Document risk assessments thoroughly
Every psychiatric SOAP note should include an assessment of risk factors like suicidal/homicidal intent.
You need this explicit screening for suicidal and homicidal ideation to establish appropriate standards of care. Assess and document both risk factors and protective factors that inform your clinical judgment.
Like with every other aspect, note any changes in risk status compared to previous visits. Then, discuss your clinical decision-making for the kind of intervention required.
It’s important to state your rationale for possible interventions considered but not implemented.
Here’s an example
Suicide risk assessment completed. Patient acknowledges passive thoughts of 'not wanting to be here anymore' but denies active suicidal ideation, plan, or intent. No history of attempts.
Protective factors include strong connection to children, religious beliefs prohibiting suicide, willingness to engage in treatment, and agreement to a safety plan. Safety plan reviewed and updated today; patient contracted to call crisis line if thoughts worsen before next appointment.
Justify medication decisions explicitly
Document your rationale for starting, continuing, adjusting, or discontinuing medications.
This will support the necessity for each medication and reduce liability.
Share your reasoning for prescribing each medication, dose adjustment, or discontinuation. You have to track the benefits and side effects of each medicine. Mention patient-reported adherence and any barriers to adherence they experience.
You can also add any medication education you’ve offered to help patients understand their role.
Here’s an example
Increasing escitalopram from 10mg to 15mg daily due to partial response (GAD-7 decreased from 18 to 12) with good tolerability after 4 weeks. Patient reports improved ability to fall asleep but continued daily anxiety symptoms interfering with work performance. Discussed potential side effects of increased dose, including possible QT prolongation; assessed benefits to outweigh risks. Patient agreeable to increase.
Addressing concerns about SOAP notes in psychiatry
I get it: You likely have some questions and concerns about implementing psychiatric SOAP notes.
Let me answer some of the most common concerns about these notes.
Concern 1: Is my patient information safe with detailed SOAP notes?
Your patient information is always protected.
While SOAP notes are more accessible than psychotherapy notes, they’re still governed by HIPAA regulations. That means only healthcare providers directly working with a patient can access these notes. You can also use a secure EHR platform to protect your notes further.
Concern 2: Will SOAP notes limit my ability to document nuanced psychiatric observations?
The SOAP note format gives you the space to capture every nuance in a patient conversation.
You can use the Assessment section to document your observations and clinical interpretation. This is your space to note observations around behavior patterns, responses to interventions, and other details.
Here’s the best part: You can customize our psychiatric SOAP notes template to match your style and maintain the depth of your observations.
Concern 3: Do SOAP notes create more documentation burden?
Done well, SOAP notes can actually reduce documentation time.
When you use a consistent template, it’s easier to organize all the insights and observations into the right sections. This way, you can document during or immediately after a session and prevent backlog.
Besides, an AI medical scribe like Freed can do all the heavy lifting on your behalf to prepare in-depth psychiatry SOAP notes.
Simply record your patient conversations with Freed, and it’ll generate detailed notes in the SOAP format. Edit them, save them to your EHR, or print them out—it’s completely up to you. Freed also deletes conversation recordings after 30 days to maintain confidentiality.
Concern 4: What should I include and exclude in my psychiatric SOAP notes?
Effective SOAP notes for psychiatry balance comprehensives with patient privacy. Let’s discuss what to include and exclude in these notes.
Include
- Relevant symptoms, behaviors, and statements that support the diagnosis
- Risk assessments, including suicidal and homicidal ideation screening
- Medication responses, side effects, and adherence information
- Objective observations of mental status and functioning
- Assessment and treatment plan with follow-ups
Exclude
- Details that could stigmatize the patient if the record were accessed
- Personal reactions to the patient that aren't clinically relevant
- Subjective judgments about character or personality
- Speculative diagnoses without supporting evidence
- Irrelevant personal details about the patient's life
Be more present for your patients and for yourself with Freed
Documentation is a double-edged sword for psychiatrists.
It’s essential for tracking patient progress and maintaining compliance. Yet, it can consume all your attention and time needed for meaningful therapeutic connection.
This impossible choice — fully engaging with patients or spending evenings on paperwork — doesn't have to be yours anymore.
Freed can be the ultimate blessing for psychiatrists.
The AI SOAP note Generator works in the background while you give patients your undivided attention. And your SOAP notes are ready before the patient even exits your clinic.
Try Freed to see how it can speed up documentation.
Your future self (and your patients) will thank you.
FAQs
Frequently asked questions from clinicians and medical practitioners.
Do psychiatrists use SOAP notes?
How to write a good psychiatry note?
What is the mental status exam in a SOAP note?
.avif)
Related content
.svg)
.svg)
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.