How to write a Treatment Plan, Types, & Examples
Let’s be honest — treatment planning is the broccoli of clinical work.
Necessary. Good for everyone. But not exactly the thing we look forward to.
You’re trying to deliver great care, keep up with documentation, and somehow finish everything before your dinner gets cold.
Most days, it feels like you’re stuck in a never-ending loop of: assess → plan → document → repeat.
But what if treatment planning didn’t have to hijack your whole evening?
I put together this guide to help you document faster without cutting corners. You’ll find practical tips and plug-and-play templates — because your brain shouldn’t have to run a marathon just to finish a progress note.
Let’s turn treatment planning from a time-sucking chore into something you can knock out like a pro.
What is a treatment plan?
A treatment plan is a detailed and personalized document outlining the process and interventions to resolve a patient’s medical condition.
Think of it like Google Maps for your patient’s care.
It shows where they are, where they need to go, and which route will avoid the most traffic (and side effects).
It’s easy to mix them up with SOAP notes — but here’s the difference:
- SOAP notes are like journal entries: documenting what happened in a single session.
- Treatment plans offer the big picture: they guide care across weeks or months.
Say you’re treating a patient with generalized anxiety disorder (GAD).
Psychiatrists will rely on some type of progress note to log specific short-term improvements in their behavioral and cognitive functioning. They can also use them to organize the next session.
A psychiatric treatment plan, in the same instance, will prioritize extended care.
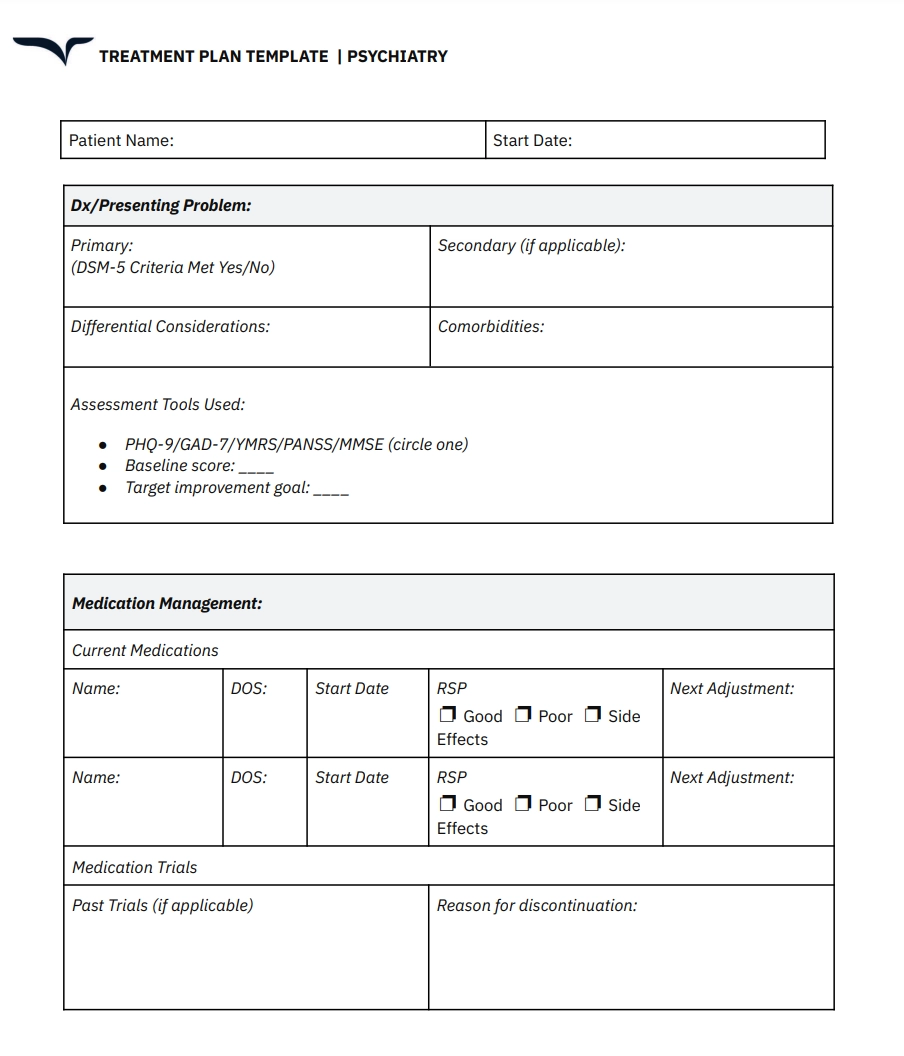
It’ll begin with a comprehensive description of the patient’s symptoms. Then, it may include elements such as:
- Long-term medication management to alleviate comorbid symptoms (depression)
- Effective coping strategies to minimize social anxiety
- Permanent lifestyle changes to address physical concerns (muscle tension, etc.)
Beyond that, clinicians can also use these outlines to record overall wellness goals alongside treatment milestones that indicate a desired outcome in the patient's condition.
What purpose does a clinical treatment plan serve?
Standard treatment plans cover these elements:
- A detailed medical history of the patient (past diagnoses, treatments, etc.)
- The current condition that they’re experiencing and how they’d like to address it
- Clear-cut, long-term clinical objectives to note crucial milestones/improvements
- A comprehensive overview of the treatment modalities the provider will target or use
- An overall review and evaluation of the patient’s progress and intervention strategies
Done right, a good treatment plan does more than check a box. It:
- Personalizes care: It outlines specific goals and methods that actually make sense for that patient—not some imaginary “textbook case.”
- Flags risks: Maybe GAD treatment includes antidepressants, but what if the patient also has hypothyroidism? That plan helps you catch the hidden red flags.
- Monitors progress: Think of it as a ruler you measure clinical success against—one goal, one intervention, one outcome at a time.
- Improves communication: When everyone knows the game plan (from patient to provider to payer) fewer things fall through the cracks.
Finally, clinical treatment plans help healthcare practitioners effectively communicate with and educate patients about their condition.
That translates to informed clinical decision-making, especially when dealing with chronic illnesses.
4 types of treatment plans you can use
Like clinical notes, treatment plans vary based on your specialty and patient scenarios. It simply means healthcare professionals can create these outlines depending on who and what they’re treating.
Here are four common treatment plans:
Medical treatment plans
Medical treatment plans are primarily directed at managing chronic or acute conditions, surgeries, and general patient care. In case of comorbidities, they may involve input from multiple specialists.
Examples: Management plan for diabetes, extended post-surgery recovery.
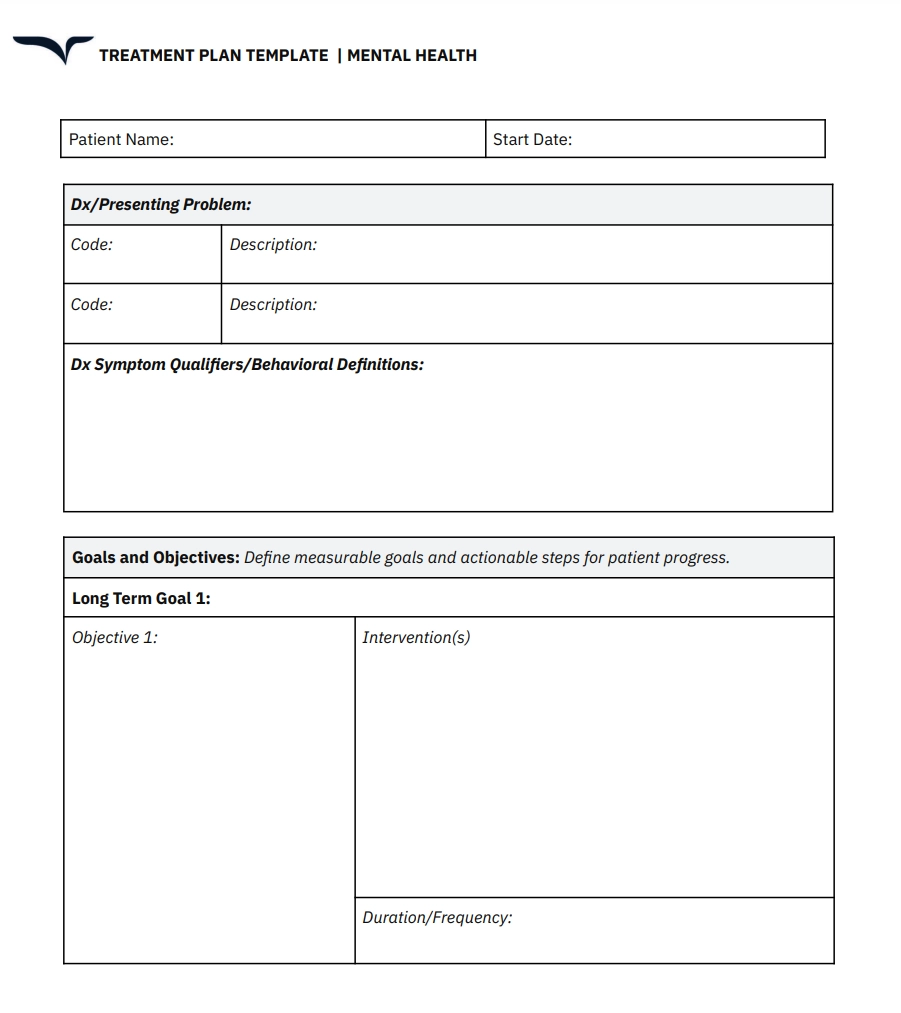
Mental health treatment plans
Mental health treatment outlines are exclusively used in non-psychiatric settings. Therapists will rely on such plans to formulate specific cognitive exercises that are tailored to their client’s needs.
Examples: Cognitive behavioral therapy (CBT) for GAD, crisis counseling, and family therapy.
Behavioral or educational treatment plans
Psychologists usually devise plans when dealing with patients with specific cognitive issues or phobias. (mysophobia/claustrophobia). Counselors also use such strategies to help students with learning disabilities or speech impediments.
Example: Individualized education programs (IEPs) for managing attention deficit hyperactivity disorder (ADHD), speech therapy, and exposure training.
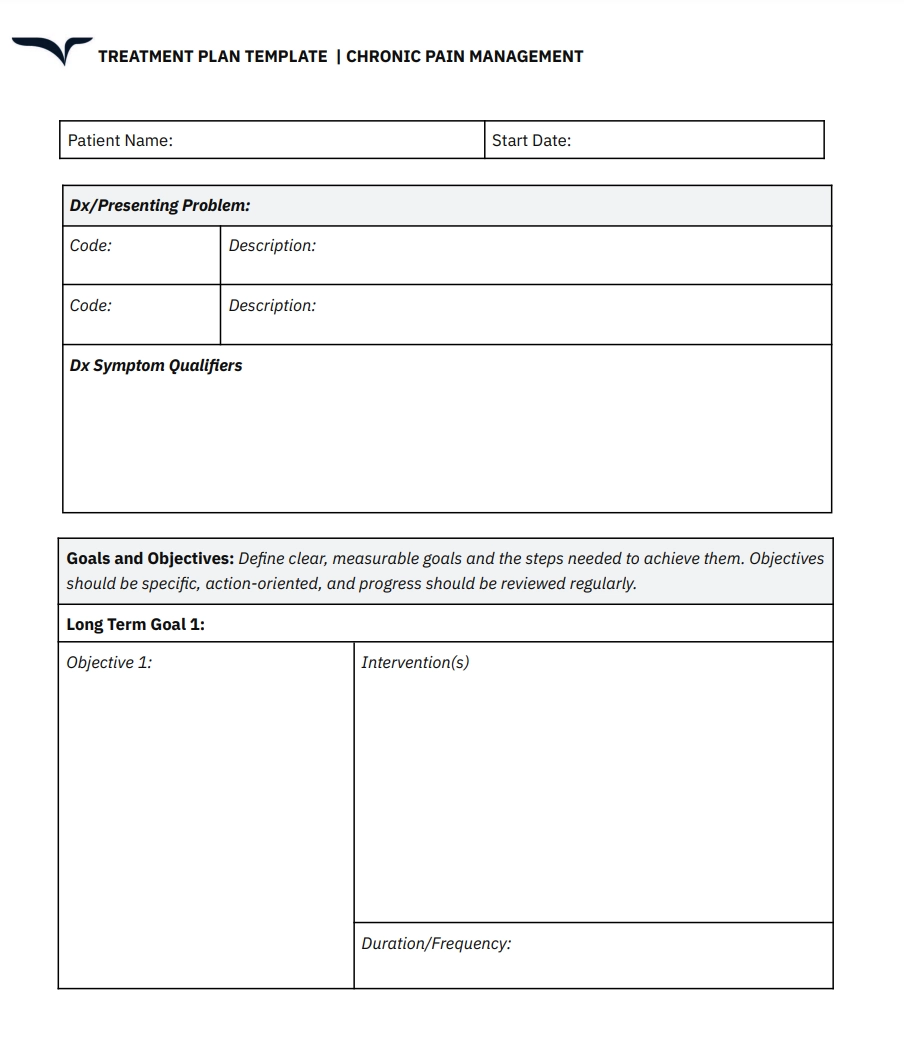
Physical therapy treatment plans
Typically, healthcare providers create physical therapy treatment plans to help patients regain physical function after severe injuries. They’re also routinely used to improve the overall quality of life for people with chronic conditions or disabilities.
Examples: Post-stroke rehabilitation and pain management exercises for arthritis.
A 4-step guide for building an effective treatment plan
Now, let’s shift our focus to how you can create a treatment plan.
We'll use a treatment framework for GAD as the standard example across all steps. Don't worry—the principles apply to any outline you might want to create.
Start by aligning patient history with the chief complaint
Sir William Osler, one of the founding professors of the Johns Hopkins Hospital, once famously said:
“The good physician treats the disease; the great physician treats the patient who has the disease.”
Put simply: A patient's clinical history and present concern(s) will always be linked. You can’t diagnose the latter without evaluating the former.
So, as a medical professional, beyond basic demographic patient information, you must also look at the their:
- Medical history (previous illnesses, injuries, surgeries, etc.)
- Family history
- Social habits and general lifestyle (frequency of exercise, alcohol consumption, etc.)
- Ongoing medications and known allergies
- Assessments from administered tests (review of systems, lab cultures, etc.)
- History of present illness (onset, severity, patient-specific modifying factors)
Once you have these down, then you assess the current condition.
For example, let’s say you’re treating a patient with GAD. A common symptom of this disorder is repetitive disturbance during sleep cycles. Incidentally, that patient also happens to have a history of sleep apnea.
How do you determine what’s causing them to wake up in the middle of the night? Is it merely an associated GAD symptom? Or is an obstructed airway the underlying problem?
More importantly, what treatment course do you recommend—CPAP therapy or muscle relaxation exercise before bed?
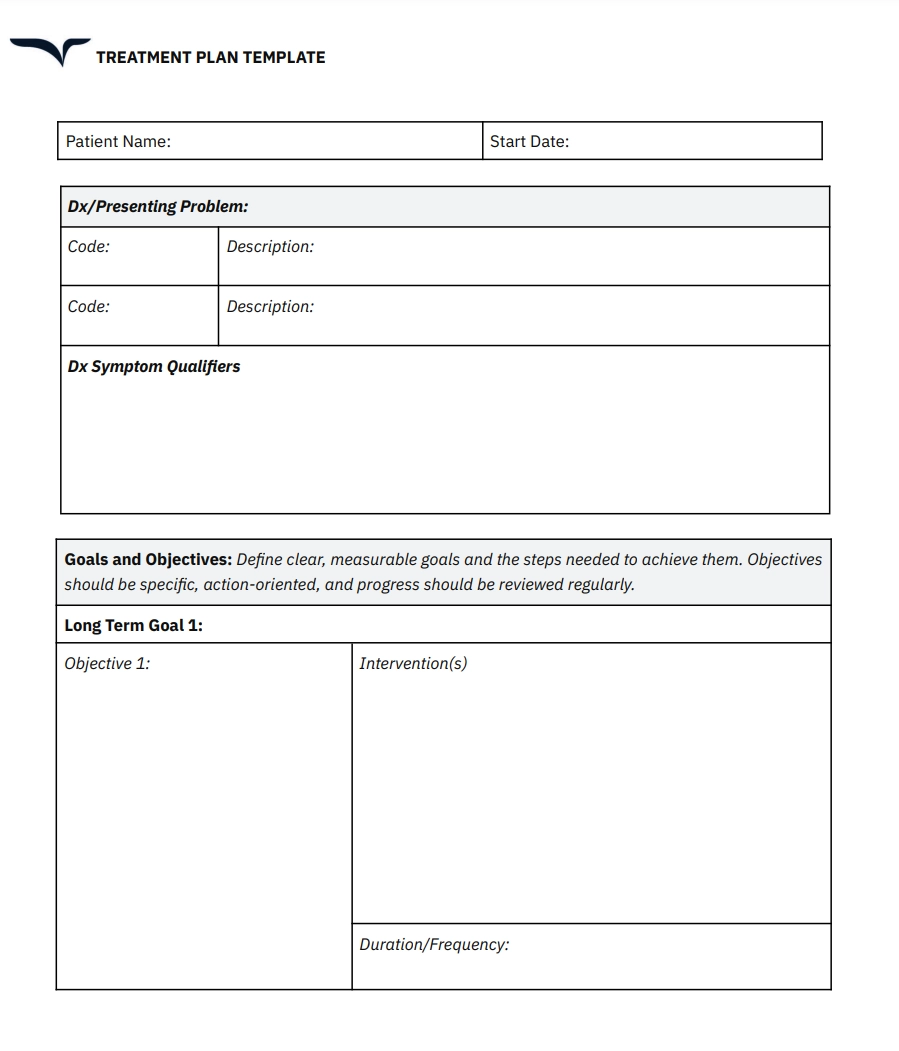
Set up a SMART goal framework
Great treatment plans are Specific, Measurable, Achievable, Relevant, and Time-bound.
Let’s look at how that translates to a treatment framework for GAD.
The first thing you’ll need to do is to break down your clinical objectives into short-term and long-term goals.
Here’s what the short-term strategy could look like:
Time frame: 0-4 months
Objectives:
- Reduce the patient’s frequency/intensity of excessive worry about daily routines. Measure by a 30% improvement on the Penn State Worry Questionnaire (PSWQ).
- Improve the patient's sleep cycle through regular exercise (15 minutes daily) and avoiding stimulants (caffeine, nicotine, etc.) before bed. Measure by comparing weekly undisturbed sleep cycles.
- Learn and engage in progressive muscle relaxation techniques daily to lower irritability, restlessness, and muscle tension. Practice at least once a day.
As for the long-term goals, they could be structured as:
Time frame: 4-16 months
Objectives:
- Achieve and maintain at least a 50% reduction in the patient’s overall anxiety levels. Measure against the GAD-7 scale (0-4 score for moderate anxiety, 5-9 for severe cases).
- Encourage building a support framework (close friends, support groups) to improve the overall quality of social interactions and interpersonal relationships.
- Develop patient-specific strategies to manage unforeseen stressors. Utilize CBT to identify behavioral tendencies that repeatedly cause anxiety.
Implementing definitive goals this way will help set realistic expectations on what clinicians and patients can achieve during the course of treatment. It also directly feeds the next step.
Assess and describe each intervention strategy individually
Once you’ve got your treatment goals, you must review and choose the modalities that offer the best possible chance of success.
Here, you’re covering two particular aspects, namely:
- A detailed description of the method/therapy you’ll use (including sub-routines)
- The frequency/dosage and duration of the process
Let's say you've decided on CBT (instead of medication) as the best approach for your patient. However, CBT is a broad treatment method that includes multiple sub-practices.
So, instead of just listing CBT as the recommended/administered treatment, you could organize your plan as follows:
Intervention/Strategy: CBT
- Cognitive restructuring to identify and reframe catastrophic thinking and irrational thoughts into a more balanced outlook.
- Psychoeducation to familiarize the patient with associated symptoms, including physical tension, dizziness, and involuntary fight-or-flight responses.
- Behavioral activation to lower avoidance tendencies and increase positive reinforcement.
Duration & Frequency:
- Short-term: 10-14 sessions that prioritize lowering general anxiety levels and learning effective coping mechanisms.
- Long-term: Ongoing consultations with therapist and relapse prevention sessions every 3-6 weeks.
Outlining the proposed methods will clarify the steps that both clinicians and patients need to take during the treatment process.
It also provides you with a direct channel for comparison. For instance, if the patient shows no improvement even after administering each proposed step, you could look into reevaluating the strategy.
Create distinct benchmarks to track progress and reevaluate when necessary
For the final step, you must consistently track patient progress and treatment milestones.
Again, going with the GAD example, this could involve:
- GAD-7 tests during designated sessions to determine symptom severity
- PSWQ assessments every 2 weeks to monitor anxiety levels during daily routines
- Weekly self-reports on anxiety-inducing incidents and the challenges they posed
- Journaling to identify repetitive occurrences of specific symptoms
Using the GAD-7 test and PSWQ assessments will help determine whether you’re meeting the clinical goals you’ve set.
Meanwhile, weekly self-reports and journaling will reveal whether the administered intervention strategy needs fine-tuning.
Notice that we've used two distinct benchmark categories.
The first (GAD-7 & PSWQ) analyzes how aligned you and the patient are with the initially proposed goals. The second (self-reports and journaling) tracks the effectiveness of the treatment method.
This could be easily applied to other conditions as well. Take diabetes management as an example. You can use the HbA1c and the oral glucose tolerance test for the first benchmark. Patient reports and home-administered insulin tests can serve as the second.
Use Freed to simplify treatment plan documentation
An organized clinical treatment plan doesn’t just describe what you intend to do for your patients.
When implemented well, they allow for effective communication, streamline administrative workflow, and (most importantly) help you achieve what you set out to do in the first place—improve lives.
With Freed's AI clinical documentation, you don’t just get a plan — you get your time, your evenings, and maybe even a little joy back.
Instantly create clinician-ready treatment outlines from your spoken notes. The best part? It effortlessly adapts to your dictation style to accurately capture critical information.
Try our AI scribe for free today!
Table of Contents
Let’s be honest — treatment planning is the broccoli of clinical work.
Necessary. Good for everyone. But not exactly the thing we look forward to.
You’re trying to deliver great care, keep up with documentation, and somehow finish everything before your dinner gets cold.
Most days, it feels like you’re stuck in a never-ending loop of: assess → plan → document → repeat.
But what if treatment planning didn’t have to hijack your whole evening?
I put together this guide to help you document faster without cutting corners. You’ll find practical tips and plug-and-play templates — because your brain shouldn’t have to run a marathon just to finish a progress note.
Let’s turn treatment planning from a time-sucking chore into something you can knock out like a pro.
What is a treatment plan?
A treatment plan is a detailed and personalized document outlining the process and interventions to resolve a patient’s medical condition.
Think of it like Google Maps for your patient’s care.
It shows where they are, where they need to go, and which route will avoid the most traffic (and side effects).
It’s easy to mix them up with SOAP notes — but here’s the difference:
- SOAP notes are like journal entries: documenting what happened in a single session.
- Treatment plans offer the big picture: they guide care across weeks or months.
Say you’re treating a patient with generalized anxiety disorder (GAD).
Psychiatrists will rely on some type of progress note to log specific short-term improvements in their behavioral and cognitive functioning. They can also use them to organize the next session.
A psychiatric treatment plan, in the same instance, will prioritize extended care.
It’ll begin with a comprehensive description of the patient’s symptoms. Then, it may include elements such as:
- Long-term medication management to alleviate comorbid symptoms (depression)
- Effective coping strategies to minimize social anxiety
- Permanent lifestyle changes to address physical concerns (muscle tension, etc.)
Beyond that, clinicians can also use these outlines to record overall wellness goals alongside treatment milestones that indicate a desired outcome in the patient's condition.
What purpose does a clinical treatment plan serve?
Standard treatment plans cover these elements:
- A detailed medical history of the patient (past diagnoses, treatments, etc.)
- The current condition that they’re experiencing and how they’d like to address it
- Clear-cut, long-term clinical objectives to note crucial milestones/improvements
- A comprehensive overview of the treatment modalities the provider will target or use
- An overall review and evaluation of the patient’s progress and intervention strategies
Done right, a good treatment plan does more than check a box. It:
- Personalizes care: It outlines specific goals and methods that actually make sense for that patient—not some imaginary “textbook case.”
- Flags risks: Maybe GAD treatment includes antidepressants, but what if the patient also has hypothyroidism? That plan helps you catch the hidden red flags.
- Monitors progress: Think of it as a ruler you measure clinical success against—one goal, one intervention, one outcome at a time.
- Improves communication: When everyone knows the game plan (from patient to provider to payer) fewer things fall through the cracks.
Finally, clinical treatment plans help healthcare practitioners effectively communicate with and educate patients about their condition.
That translates to informed clinical decision-making, especially when dealing with chronic illnesses.
4 types of treatment plans you can use
Like clinical notes, treatment plans vary based on your specialty and patient scenarios. It simply means healthcare professionals can create these outlines depending on who and what they’re treating.
Here are four common treatment plans:
Medical treatment plans
Medical treatment plans are primarily directed at managing chronic or acute conditions, surgeries, and general patient care. In case of comorbidities, they may involve input from multiple specialists.
Examples: Management plan for diabetes, extended post-surgery recovery.
Mental health treatment plans
Mental health treatment outlines are exclusively used in non-psychiatric settings. Therapists will rely on such plans to formulate specific cognitive exercises that are tailored to their client’s needs.
Examples: Cognitive behavioral therapy (CBT) for GAD, crisis counseling, and family therapy.
Behavioral or educational treatment plans
Psychologists usually devise plans when dealing with patients with specific cognitive issues or phobias. (mysophobia/claustrophobia). Counselors also use such strategies to help students with learning disabilities or speech impediments.
Example: Individualized education programs (IEPs) for managing attention deficit hyperactivity disorder (ADHD), speech therapy, and exposure training.
Physical therapy treatment plans
Typically, healthcare providers create physical therapy treatment plans to help patients regain physical function after severe injuries. They’re also routinely used to improve the overall quality of life for people with chronic conditions or disabilities.
Examples: Post-stroke rehabilitation and pain management exercises for arthritis.
A 4-step guide for building an effective treatment plan
Now, let’s shift our focus to how you can create a treatment plan.
We'll use a treatment framework for GAD as the standard example across all steps. Don't worry—the principles apply to any outline you might want to create.
Start by aligning patient history with the chief complaint
Sir William Osler, one of the founding professors of the Johns Hopkins Hospital, once famously said:
“The good physician treats the disease; the great physician treats the patient who has the disease.”
Put simply: A patient's clinical history and present concern(s) will always be linked. You can’t diagnose the latter without evaluating the former.
So, as a medical professional, beyond basic demographic patient information, you must also look at the their:
- Medical history (previous illnesses, injuries, surgeries, etc.)
- Family history
- Social habits and general lifestyle (frequency of exercise, alcohol consumption, etc.)
- Ongoing medications and known allergies
- Assessments from administered tests (review of systems, lab cultures, etc.)
- History of present illness (onset, severity, patient-specific modifying factors)
Once you have these down, then you assess the current condition.
For example, let’s say you’re treating a patient with GAD. A common symptom of this disorder is repetitive disturbance during sleep cycles. Incidentally, that patient also happens to have a history of sleep apnea.
How do you determine what’s causing them to wake up in the middle of the night? Is it merely an associated GAD symptom? Or is an obstructed airway the underlying problem?
More importantly, what treatment course do you recommend—CPAP therapy or muscle relaxation exercise before bed?
Set up a SMART goal framework
Great treatment plans are Specific, Measurable, Achievable, Relevant, and Time-bound.
Let’s look at how that translates to a treatment framework for GAD.
The first thing you’ll need to do is to break down your clinical objectives into short-term and long-term goals.
Here’s what the short-term strategy could look like:
Time frame: 0-4 months
Objectives:
- Reduce the patient’s frequency/intensity of excessive worry about daily routines. Measure by a 30% improvement on the Penn State Worry Questionnaire (PSWQ).
- Improve the patient's sleep cycle through regular exercise (15 minutes daily) and avoiding stimulants (caffeine, nicotine, etc.) before bed. Measure by comparing weekly undisturbed sleep cycles.
- Learn and engage in progressive muscle relaxation techniques daily to lower irritability, restlessness, and muscle tension. Practice at least once a day.
As for the long-term goals, they could be structured as:
Time frame: 4-16 months
Objectives:
- Achieve and maintain at least a 50% reduction in the patient’s overall anxiety levels. Measure against the GAD-7 scale (0-4 score for moderate anxiety, 5-9 for severe cases).
- Encourage building a support framework (close friends, support groups) to improve the overall quality of social interactions and interpersonal relationships.
- Develop patient-specific strategies to manage unforeseen stressors. Utilize CBT to identify behavioral tendencies that repeatedly cause anxiety.
Implementing definitive goals this way will help set realistic expectations on what clinicians and patients can achieve during the course of treatment. It also directly feeds the next step.
Assess and describe each intervention strategy individually
Once you’ve got your treatment goals, you must review and choose the modalities that offer the best possible chance of success.
Here, you’re covering two particular aspects, namely:
- A detailed description of the method/therapy you’ll use (including sub-routines)
- The frequency/dosage and duration of the process
Let's say you've decided on CBT (instead of medication) as the best approach for your patient. However, CBT is a broad treatment method that includes multiple sub-practices.
So, instead of just listing CBT as the recommended/administered treatment, you could organize your plan as follows:
Intervention/Strategy: CBT
- Cognitive restructuring to identify and reframe catastrophic thinking and irrational thoughts into a more balanced outlook.
- Psychoeducation to familiarize the patient with associated symptoms, including physical tension, dizziness, and involuntary fight-or-flight responses.
- Behavioral activation to lower avoidance tendencies and increase positive reinforcement.
Duration & Frequency:
- Short-term: 10-14 sessions that prioritize lowering general anxiety levels and learning effective coping mechanisms.
- Long-term: Ongoing consultations with therapist and relapse prevention sessions every 3-6 weeks.
Outlining the proposed methods will clarify the steps that both clinicians and patients need to take during the treatment process.
It also provides you with a direct channel for comparison. For instance, if the patient shows no improvement even after administering each proposed step, you could look into reevaluating the strategy.
Create distinct benchmarks to track progress and reevaluate when necessary
For the final step, you must consistently track patient progress and treatment milestones.
Again, going with the GAD example, this could involve:
- GAD-7 tests during designated sessions to determine symptom severity
- PSWQ assessments every 2 weeks to monitor anxiety levels during daily routines
- Weekly self-reports on anxiety-inducing incidents and the challenges they posed
- Journaling to identify repetitive occurrences of specific symptoms
Using the GAD-7 test and PSWQ assessments will help determine whether you’re meeting the clinical goals you’ve set.
Meanwhile, weekly self-reports and journaling will reveal whether the administered intervention strategy needs fine-tuning.
Notice that we've used two distinct benchmark categories.
The first (GAD-7 & PSWQ) analyzes how aligned you and the patient are with the initially proposed goals. The second (self-reports and journaling) tracks the effectiveness of the treatment method.
This could be easily applied to other conditions as well. Take diabetes management as an example. You can use the HbA1c and the oral glucose tolerance test for the first benchmark. Patient reports and home-administered insulin tests can serve as the second.
Use Freed to simplify treatment plan documentation
An organized clinical treatment plan doesn’t just describe what you intend to do for your patients.
When implemented well, they allow for effective communication, streamline administrative workflow, and (most importantly) help you achieve what you set out to do in the first place—improve lives.
With Freed's AI clinical documentation, you don’t just get a plan — you get your time, your evenings, and maybe even a little joy back.
Instantly create clinician-ready treatment outlines from your spoken notes. The best part? It effortlessly adapts to your dictation style to accurately capture critical information.
Try our AI scribe for free today!
FAQs
Frequently asked questions from clinicians and medical practitioners.
How do you write a treatment plan?
What are examples of treatment plans?
What are the four elements of a treatment plan?
How specific should my treatment plan goals be?

Related content
.svg)
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.