9 Clinical Note Templates and Examples for Every Setting
It’s the same equation for any kind of documentation:
Poor structure + Poor consistency = chaos.
Clinical social worker, Beth Rontal (AKA the Documentation Wizard) wrote about the striking resemblance between clinical notes and dirty dishes.
Rontal says that they both:
- Start as a mess
- Are never-ending repetitive tasks
- Are easy to put off
- Are as necessary as they are tedious.
But just like dishes, notes matter.
That's where clinical note templates come in.
A good note template saves time and cuts through the mental clutter after each session.
Why use clinical note templates
Clinical documentation isn’t the time to reinvent the wheel — or test your creative writing skills.
With clinical note templates, it becomes easier to cut out the fluff and self-edit. You get:
- Efficiency: Speed up documentation by helping you focus on essential information and cut down on mental fatigue
- Consistency: Provide a structure that keeps your notes complete and easy to read.
- Compliance: Standardize your notes in alignment with legal and insurance requirements so you can protect your patients and all care team members.
- Happier patients: Find a sweet spot for your notes that both simplifies care team coordination while giving patients themselves adequate insight into their journey with you.
But of course, clinical note templates aren’t one-size-fits-all.
The key is finding or customizing one that matches your specialty, preferred workflows, and the needs of your employer or medical institution.
9 clinical note templates & examples
Every clinical note has a purpose, each geared toward helping clinicians capture the right information in different settings.
Here’s a breakdown of the most common types:
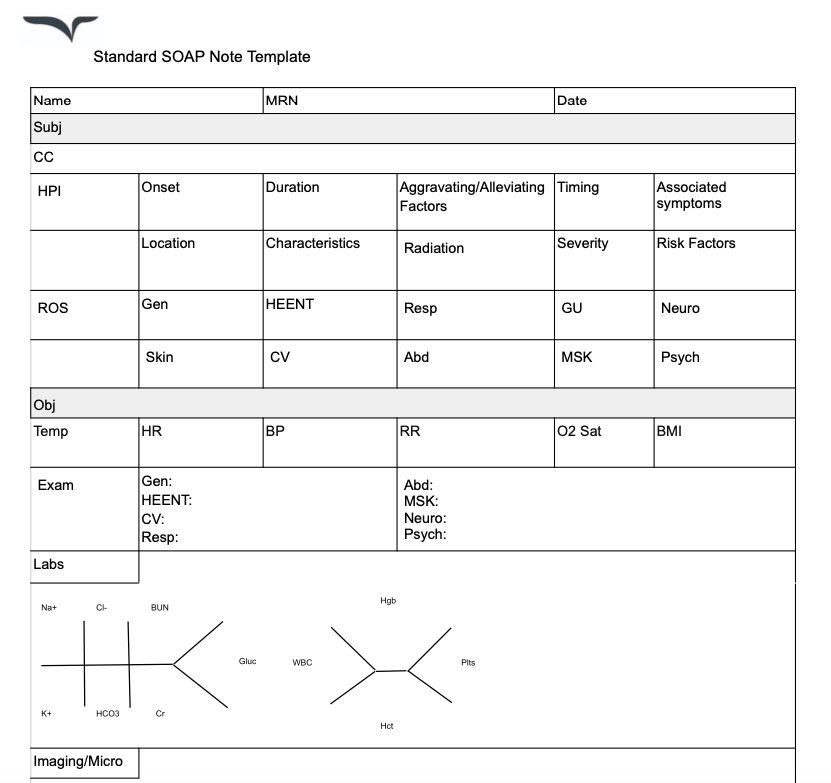
1. Progress notes
Progress notes document a patient’s status and response to treatment.
They come in many formats — with the most popular ones being the SOAP, BIRP and DAP note formats. These notes provide a complete overview of a patient’s interaction with care team members, so balancing brevity and comprehensiveness is key.
When do you use progress notes?
Different progress note templates help different healthcare environments.
The most widely used format, SOAP notes, is used in all medical, therapy, and social work settings. But others can be tailored for specific purposes — like the BIRP format for behavioral health cases.
Progress note template
Download this free progress note template today.
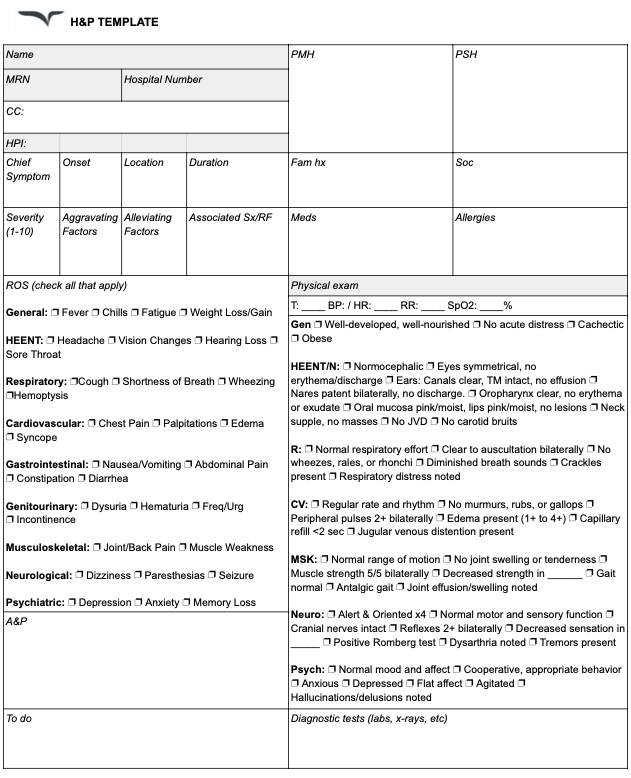
2. History & Physical (H&P) notes
H&P notes help physicians, physician assistants, and nurses summarize a patient’s medical history and physical exam findings. These notes help kick off diagnosis and treatment planning by offering care teams a detailed look at a patient’s current condition.
When do you use H&P notes?
These notes are primarily used in hospitals, primary care, and specialty clinics when admitting new patients or conducting comprehensive medical evaluations.
H&P note template
Download this free H&P clinical note template.
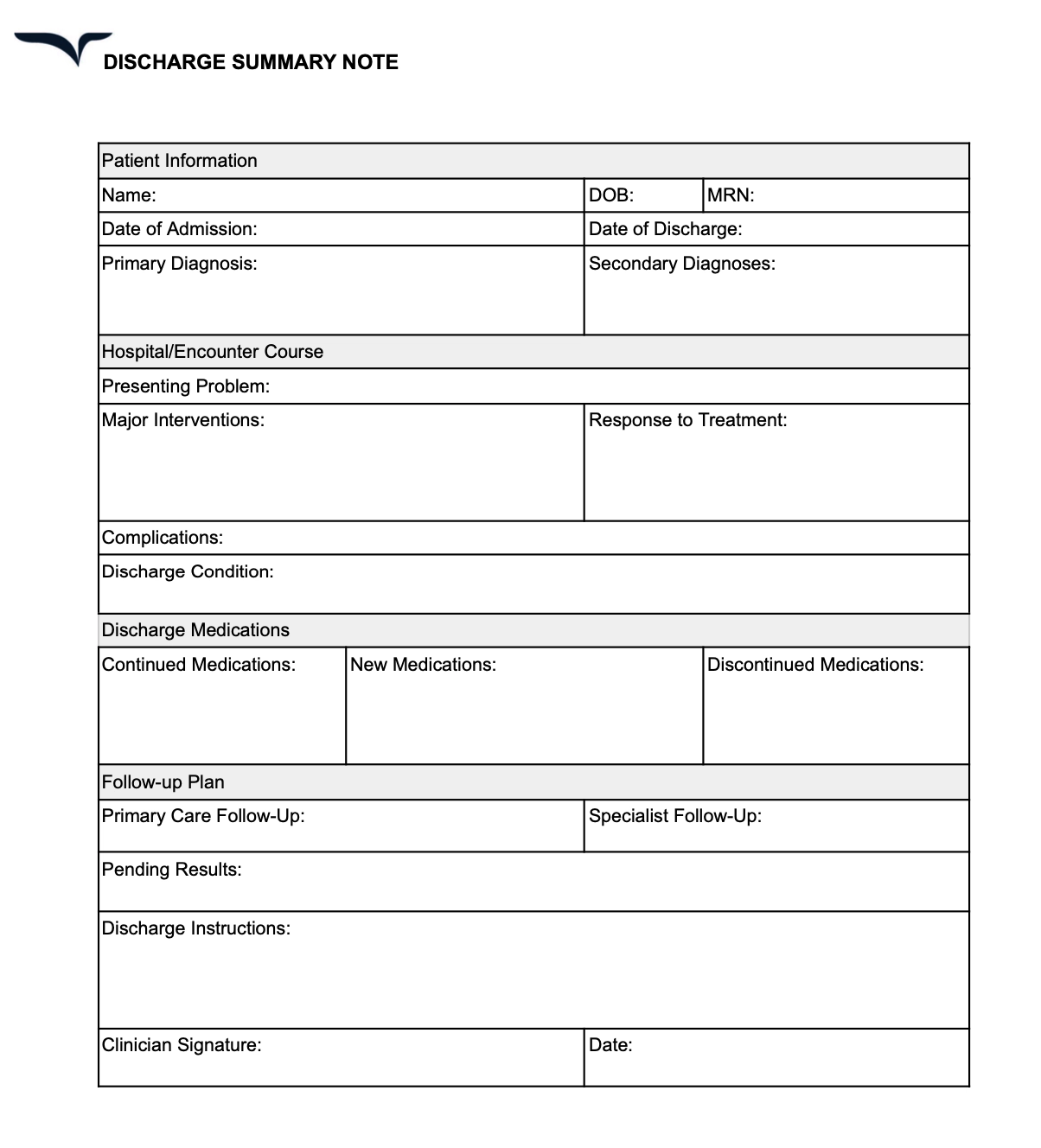
3. Discharge summaries
Discharge summaries summarize important information captured during a patient’s hospital stay — like their diagnosis, treatment, and progress during that period a team.
A discharge summary also contains instructions for post-discharge care to ensure a smooth transition over to caretakers or other healthcare providers.
When do you use discharge summaries?
Discharge summaries are required when a patient is discharged from a hospital, rehab center, or skilled nursing facility to ensure continuity of care.
Discharge summary note template
Download this free clinical note template.
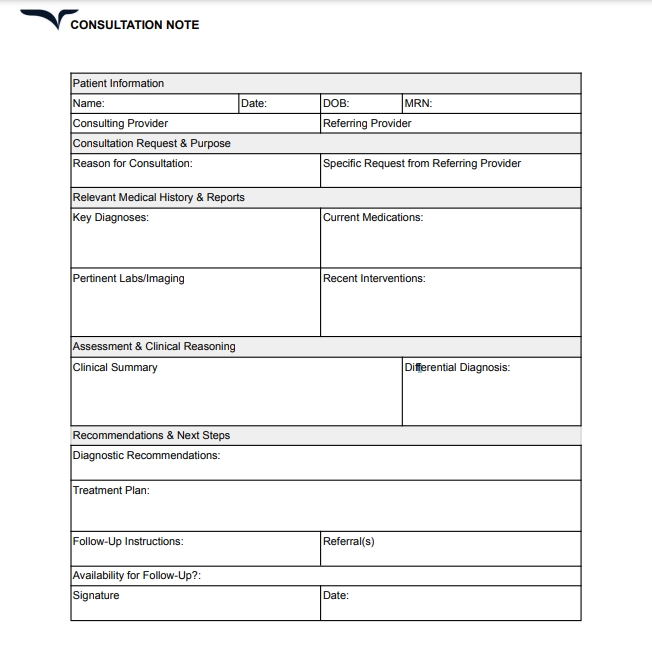
4. Consultation notes
Consultation notes contain the findings and recommendations of a specialist after evaluating a patient at the request of another provider.
These notes guide treatment decisions, align decision-making, and ensure proper continuity of care when multiple healthcare providers are involved.
When do you use consultation notes?
These notes are needed when a patient is referred to a specialist for further evaluation. They are commonly used in specialty clinics, hospitals, and multidisciplinary care settings where multiple providers collaborate on a patient’s treatment plan.
Consultation note template
Download this free consultation note template.
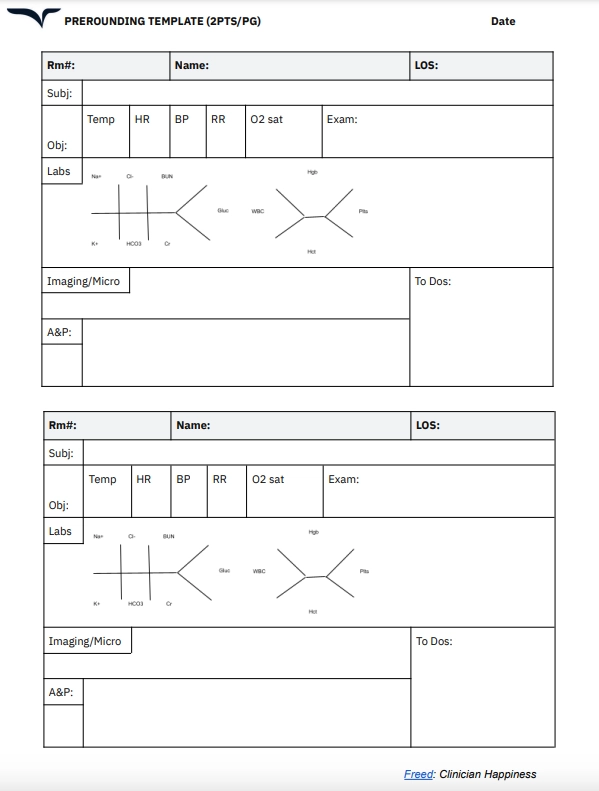
5. Prerounding notes
Prerounding notes provide a quick summary of a patient’s overnight status, lab results, and any outstanding issues.
These notes help students, interns, and junior clinicians prepare for patient discussions and streamline communication with attending physicians.
When do you use prerounding notes?
These notes are used in hospital inpatient settings before morning rounds or formal rounds by medical students, residents, and interns.
Prerounding note template
Download this new template for Prerounding.
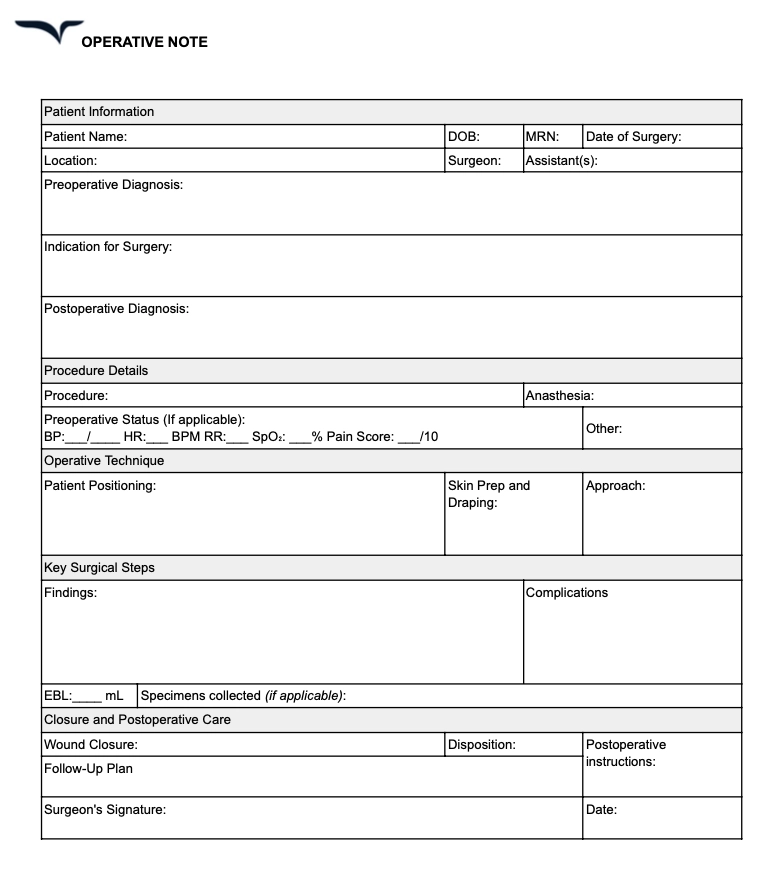
6. Operative notes
Operative notes outline the details of a surgical procedure, including the techniques used, intraoperative findings, and post-operative care instructions. Operative notes are typically written by surgeons but are sometimes co-signed by assistants, anesthesiologists, or surgical residents.
When do you use operative notes?
These notes are used in operating rooms, surgical centers, and hospitals immediately following a surgical procedure.
Operative note template
Download this free operative note template.
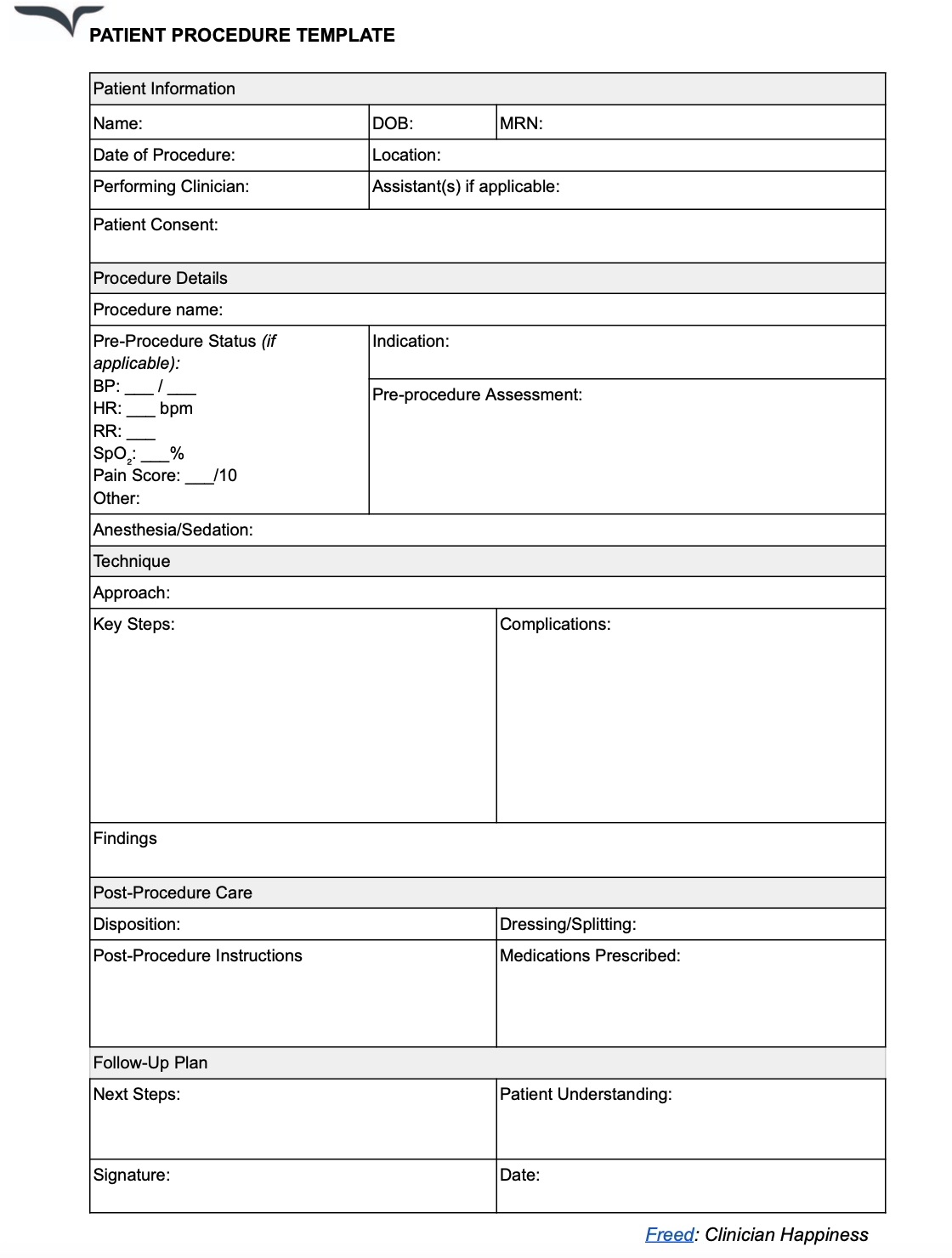
7. Procedure notes
Procedure notes document the details of non-surgical procedures — such as biopsies, endoscopies, catheter placements, or injections.
They ensure accurate record-keeping of minor procedures by capturing information such as the reason for the reason for the procedure, methods and equipment used, patient response and side effects, and post-procedure care.
When do you use procedure notes?
These notes are used in hospitals, outpatient clinics, and primary care settings immediately after performing a medical procedure.
Procedure note template
Download this procedure note template for medical treatment.
8. Nursing notes
Nursing notes (sometimes called a patient or client report) track:
- Patient assessments
- Interventions
- Responses to care
All during a shift. These ensure continuity between nurses and other healthcare providers to accurately track patient progress over time.
These notes can also follow standard progress note formats such as SOAP, DAP, and PIE.
When do you use nursing notes?
These notes are used in hospitals, long-term care facilities, and home health settings to document ongoing nursing care.
Nursing note template
Download this new template for patient client reports.

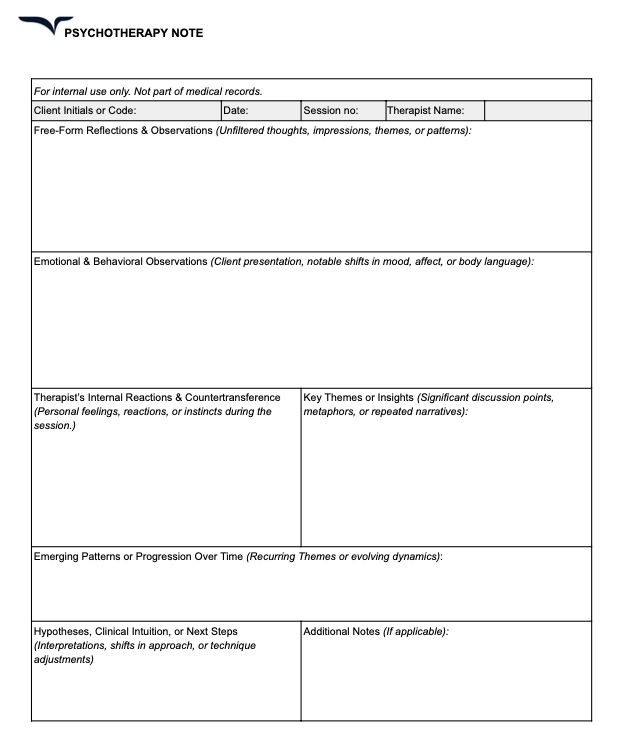
9. Psychotherapy notes
Psychotherapy notes, also called process notes, are private reflections or observations that mental health professionals after a session.
Unlike progress notes, they are not part of official medical records and cannot be used for insurance or legal purposes.
When do you use psychotherapy notes?
These notes are used by psychologists, counselors, and social workers in mental health for personal tracking of therapy sessions.
As they’re intended for private use, therapists can improve client care through deep, detailed reflections without having to worry about reviews from external parties.
Psychotherapy note template
Download this new template for mental health practitioners.
Customizing your clinical note template
Your clinical note templates are only as useful as how you use them. The key? Small tweaks to match your workflow:
Here are a few tips:
- Keep it short & structured – Use your format and stick to it, and only add relevant information.
“I think there are three important acronyms for note taking: DAP - Data, Assessment, Plan SOAP- Subjective, Objective, Assessment, Plan And KISS Keep It Short and Simple,” Reddit user MarcusArtorius
- Adapt to your setting – Some notes need details, others just the essentials. A therapy progress note template looks different than a treatment plan.
- Use bullet points – Faster to write, easier to read.
“Bullet points. Seriously. Use templates to sort the sections with the bullet points ready to go underneath each header. — Reddit user Freemind323
- Save common phrases – Dotphrases in your EHR can be a lifesaver.
- Duplicate & edit – No need to rewrite every note—just update the essentials.
"I import the old note and change/update anything that isn't accurate for that session... Fresh writing is probably 3-5 sentences per note, more if something complex is happening." — Reddit user, AntiqueOwl1662
How to choose the right clinical note template
Beyond the adjustments you can make to your note-taking process, you also need to consider the template itself.
The last thing you want to do is spend an extra hour reentering or reformatting your notes because you used a template that didn’t exactly fit the needs of your care team or employer.
Here are some best practices to help you make an informed decision:
- Match the template to your workflow: Choose a template that aligns with your day-to-day routines and habits. For example, you can opt for more structured templates if you typically have a heavier workload or less structured ones if you’re already familiar with note-writing and have a preferred writing style in place.
- Be consistent with your team: If you’re coordinating care with a team or multiple providers, opt for a template that’s aligned with the requirements or recommendations of everyone you work with. It should include mandatory details for your employer’s legal, insurance, and reimbursement needs.
- Evaluate customization options: Look for templates that allow easy modifications so you can tailor sections based on your preferences and patient needs — better yet, if it’s automated. AI notetakers like Freed, for instance, learn from your edits to transcriptions and delivers customized notes that match your style and format.
- Test and iterate: If a template isn’t working, don’t wait to adjust or switch to a different format! Try out a template for a few weeks and gather feedback from your team.
Put clinical note templates to action
Clinical notes don’t have to be a source of frustration. The right template can turn documentation from a chaotic mess into a streamlined, structured process that saves time and mental energy.
Whether you’re jotting down progress notes, discharge summaries, or mental health reflections, a well-chosen template helps you stay efficient, compliant, and focused on what matters.
And if you want to take things a step further, AI-powered tools like Freed can adapt to your style, making note-taking even more effortless.
At the end of the day, documentation should work for you — not the other way around.
Sign up for a free trial — no credit card required!
Table of Contents
It’s the same equation for any kind of documentation:
Poor structure + Poor consistency = chaos.
Clinical social worker, Beth Rontal (AKA the Documentation Wizard) wrote about the striking resemblance between clinical notes and dirty dishes.
Rontal says that they both:
- Start as a mess
- Are never-ending repetitive tasks
- Are easy to put off
- Are as necessary as they are tedious.
But just like dishes, notes matter.
That's where clinical note templates come in.
A good note template saves time and cuts through the mental clutter after each session.
Why use clinical note templates
Clinical documentation isn’t the time to reinvent the wheel — or test your creative writing skills.
With clinical note templates, it becomes easier to cut out the fluff and self-edit. You get:
- Efficiency: Speed up documentation by helping you focus on essential information and cut down on mental fatigue
- Consistency: Provide a structure that keeps your notes complete and easy to read.
- Compliance: Standardize your notes in alignment with legal and insurance requirements so you can protect your patients and all care team members.
- Happier patients: Find a sweet spot for your notes that both simplifies care team coordination while giving patients themselves adequate insight into their journey with you.
But of course, clinical note templates aren’t one-size-fits-all.
The key is finding or customizing one that matches your specialty, preferred workflows, and the needs of your employer or medical institution.
9 clinical note templates & examples
Every clinical note has a purpose, each geared toward helping clinicians capture the right information in different settings.
Here’s a breakdown of the most common types:
1. Progress notes
Progress notes document a patient’s status and response to treatment.
They come in many formats — with the most popular ones being the SOAP, BIRP and DAP note formats. These notes provide a complete overview of a patient’s interaction with care team members, so balancing brevity and comprehensiveness is key.
When do you use progress notes?
Different progress note templates help different healthcare environments.
The most widely used format, SOAP notes, is used in all medical, therapy, and social work settings. But others can be tailored for specific purposes — like the BIRP format for behavioral health cases.
Progress note template
Download this free progress note template today.
2. History & Physical (H&P) notes
H&P notes help physicians, physician assistants, and nurses summarize a patient’s medical history and physical exam findings. These notes help kick off diagnosis and treatment planning by offering care teams a detailed look at a patient’s current condition.
When do you use H&P notes?
These notes are primarily used in hospitals, primary care, and specialty clinics when admitting new patients or conducting comprehensive medical evaluations.
H&P note template
Download this free H&P clinical note template.
3. Discharge summaries
Discharge summaries summarize important information captured during a patient’s hospital stay — like their diagnosis, treatment, and progress during that period a team.
A discharge summary also contains instructions for post-discharge care to ensure a smooth transition over to caretakers or other healthcare providers.
When do you use discharge summaries?
Discharge summaries are required when a patient is discharged from a hospital, rehab center, or skilled nursing facility to ensure continuity of care.
Discharge summary note template
Download this free clinical note template.
4. Consultation notes
Consultation notes contain the findings and recommendations of a specialist after evaluating a patient at the request of another provider.
These notes guide treatment decisions, align decision-making, and ensure proper continuity of care when multiple healthcare providers are involved.
When do you use consultation notes?
These notes are needed when a patient is referred to a specialist for further evaluation. They are commonly used in specialty clinics, hospitals, and multidisciplinary care settings where multiple providers collaborate on a patient’s treatment plan.
Consultation note template
Download this free consultation note template.
5. Prerounding notes
Prerounding notes provide a quick summary of a patient’s overnight status, lab results, and any outstanding issues.
These notes help students, interns, and junior clinicians prepare for patient discussions and streamline communication with attending physicians.
When do you use prerounding notes?
These notes are used in hospital inpatient settings before morning rounds or formal rounds by medical students, residents, and interns.
Prerounding note template
Download this new template for Prerounding.
6. Operative notes
Operative notes outline the details of a surgical procedure, including the techniques used, intraoperative findings, and post-operative care instructions. Operative notes are typically written by surgeons but are sometimes co-signed by assistants, anesthesiologists, or surgical residents.
When do you use operative notes?
These notes are used in operating rooms, surgical centers, and hospitals immediately following a surgical procedure.
Operative note template
Download this free operative note template.
7. Procedure notes
Procedure notes document the details of non-surgical procedures — such as biopsies, endoscopies, catheter placements, or injections.
They ensure accurate record-keeping of minor procedures by capturing information such as the reason for the reason for the procedure, methods and equipment used, patient response and side effects, and post-procedure care.
When do you use procedure notes?
These notes are used in hospitals, outpatient clinics, and primary care settings immediately after performing a medical procedure.
Procedure note template
Download this procedure note template for medical treatment.
8. Nursing notes
Nursing notes (sometimes called a patient or client report) track:
- Patient assessments
- Interventions
- Responses to care
All during a shift. These ensure continuity between nurses and other healthcare providers to accurately track patient progress over time.
These notes can also follow standard progress note formats such as SOAP, DAP, and PIE.
When do you use nursing notes?
These notes are used in hospitals, long-term care facilities, and home health settings to document ongoing nursing care.
Nursing note template
Download this new template for patient client reports.
9. Psychotherapy notes
Psychotherapy notes, also called process notes, are private reflections or observations that mental health professionals after a session.
Unlike progress notes, they are not part of official medical records and cannot be used for insurance or legal purposes.
When do you use psychotherapy notes?
These notes are used by psychologists, counselors, and social workers in mental health for personal tracking of therapy sessions.
As they’re intended for private use, therapists can improve client care through deep, detailed reflections without having to worry about reviews from external parties.
Psychotherapy note template
Download this new template for mental health practitioners.
Customizing your clinical note template
Your clinical note templates are only as useful as how you use them. The key? Small tweaks to match your workflow:
Here are a few tips:
- Keep it short & structured – Use your format and stick to it, and only add relevant information.
“I think there are three important acronyms for note taking: DAP - Data, Assessment, Plan SOAP- Subjective, Objective, Assessment, Plan And KISS Keep It Short and Simple,” Reddit user MarcusArtorius
- Adapt to your setting – Some notes need details, others just the essentials. A therapy progress note template looks different than a treatment plan.
- Use bullet points – Faster to write, easier to read.
“Bullet points. Seriously. Use templates to sort the sections with the bullet points ready to go underneath each header. — Reddit user Freemind323
- Save common phrases – Dotphrases in your EHR can be a lifesaver.
- Duplicate & edit – No need to rewrite every note—just update the essentials.
"I import the old note and change/update anything that isn't accurate for that session... Fresh writing is probably 3-5 sentences per note, more if something complex is happening." — Reddit user, AntiqueOwl1662
How to choose the right clinical note template
Beyond the adjustments you can make to your note-taking process, you also need to consider the template itself.
The last thing you want to do is spend an extra hour reentering or reformatting your notes because you used a template that didn’t exactly fit the needs of your care team or employer.
Here are some best practices to help you make an informed decision:
- Match the template to your workflow: Choose a template that aligns with your day-to-day routines and habits. For example, you can opt for more structured templates if you typically have a heavier workload or less structured ones if you’re already familiar with note-writing and have a preferred writing style in place.
- Be consistent with your team: If you’re coordinating care with a team or multiple providers, opt for a template that’s aligned with the requirements or recommendations of everyone you work with. It should include mandatory details for your employer’s legal, insurance, and reimbursement needs.
- Evaluate customization options: Look for templates that allow easy modifications so you can tailor sections based on your preferences and patient needs — better yet, if it’s automated. AI notetakers like Freed, for instance, learn from your edits to transcriptions and delivers customized notes that match your style and format.
- Test and iterate: If a template isn’t working, don’t wait to adjust or switch to a different format! Try out a template for a few weeks and gather feedback from your team.
Put clinical note templates to action
Clinical notes don’t have to be a source of frustration. The right template can turn documentation from a chaotic mess into a streamlined, structured process that saves time and mental energy.
Whether you’re jotting down progress notes, discharge summaries, or mental health reflections, a well-chosen template helps you stay efficient, compliant, and focused on what matters.
And if you want to take things a step further, AI-powered tools like Freed can adapt to your style, making note-taking even more effortless.
At the end of the day, documentation should work for you — not the other way around.
Sign up for a free trial — no credit card required!
FAQs
Frequently asked questions from clinicians and medical practitioners.
What’s considered a clinical note?
What are the three most common types of progress notes?
What’s the difference between SOAP, DAP, and other progress note formats?
What are the different types of clinical notes for therapy?
.avif)
Related content
.svg)
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.