How to Write Clinical Notes Faster—5 Easy Steps
Three things can be true:
- Clinical notes are the building blocks of any patient's medical record.
- With a good clinical note, we can easily monitor a patient's progress and outline a plan of care.
- They're also an overwhelming pain.
Let's face it: clinical documentation is no ones favorite part of the job. But they don't have to keep you up at night (literally).
There has to be a better way, and turns out: there is.
We've scoured forums and our personal network for tips from healthcare providers on how to:
- Quickly (and accurately) write clinical documentation;
- Avoid note bloat and prioritize important structured data;
- Ensure compliance in your medical records.
- Never take your notes home again.
Let's get started.
How to write clinical notes—a step-by-step guide
These notes are going down.
Here's a step-by-step guide on how to quickly write clinical notes while preserving key information.
1. Choose a framework or note template
First, you need to decide which format suits you best.
I'm sure your no stranger to the standard note templates:
- SOAP notes (or APSO)
- DAP notes
- BIRP notes
The choice really comes down to what you need to do with the information.
SOAP notes
SOAP (Subjective, Objective, Assessment, Plan) notes are a classic choice that works well for most clinical settings.
The four key components are:
- The patient’s report (Subjective);
- Your observations (Objective);
- Your evaluation (Assessment);
- The treatment plan (Plan).
It's a comprehensive clinical note type that's great for monitoring patient's progress and plan of care.
“I find that keeping the SOAP format-Subjective, Objective, Assessment, and Plan-keeps my notes organized and concise for other healthcare providers to more quickly comprehend the status and plan regarding the patient.” — Dr. Sham Singh, Winit Clinic
DAP notes
DAP notes (Data, Assessment, Plan) offer a more straightforward approach.
Unlike SOAP, which separates subjective and objective information, DAP notes combine both into a single section labeled "Data."
This patient data section provides a detailed description of the patient's symptoms and other relevant information.
BIRP notes
BIRP notes (Behavior, Intervention, Response, Plan) are best for mental health professionals.
They let you track:
- The patient’s behavior;
- What interventions you tried;
- How the patient responded;
- What’s next.
This framework helps capture detailed observations and responses, which is crucial for ongoing mental health care.
2. Make a list of must-have components
These frameworks are grate for structuring your notes. Now, we need to see what clinical information actually matters.
- Chief complaint: the main issue or reason the patient is seeking care.
- Review of systems (ROS): symptoms the patient is experiencing.
- Past medical history (PMH or Pmhx): Record any relevant past medical conditions, surgeries, or hospitalizations that could impact the current treatment.
- Medication history: list current medications, including dosages and any known allergies or adverse reactions. Tip: only focus on what's relevant.
- Physical examination findings: the results of your physical examination.
- Exam results: any lab results, imaging studies, or other diagnostic tests that were performed.
- Plan: further actions including the treatment plan, additional tests, and follow-up appointments.
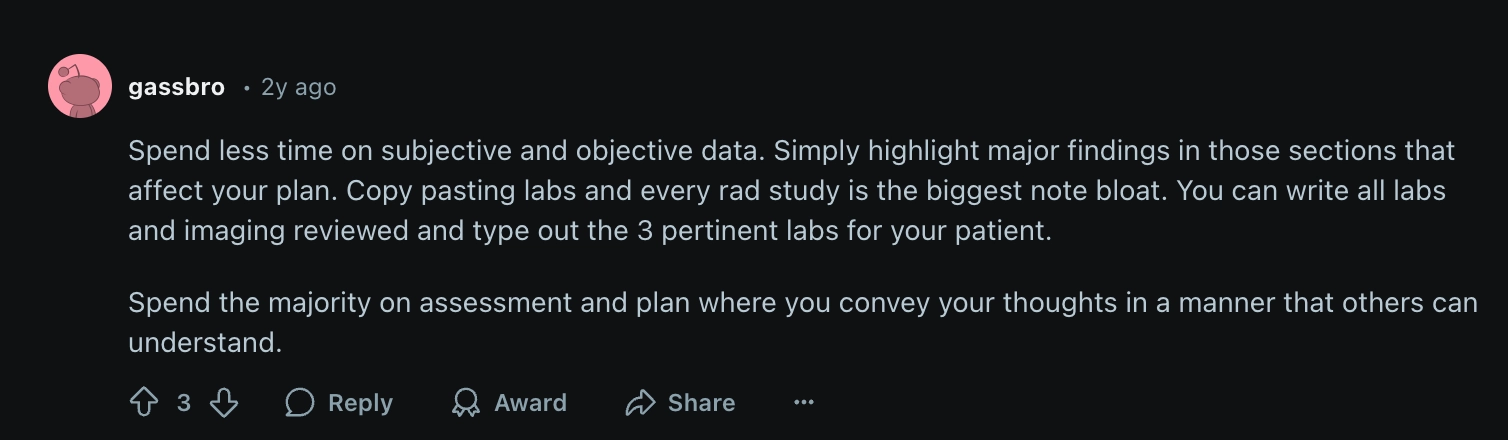
💡 Tip: Focus on major findings and don't worry about copy/pasting every detail or full lab.
3. Lean on medical abbreviations
Is it a short cut or a lifeline?
Medical abbreviations in your notes will save you a lot of time.
Here are some abbreviations to get you to the finish line.
- BP — Blood Pressure
- HR — Heart Rate
- C/O — Complains Of
- WNL — Within Normal Limits
- Rx — Prescription
- H&P — History and Physical
- PMH — Past Medical History
- Dx — Diagnosis
It wouldn't hurt to look up some more medical abbreviations in medical textbooks or online medical dictionaries.
💡 Tip: There are online databases with comprehensive lists of standardized terminology and shorthands. Bookmark one for easy access.
4. Use an AI scribe
Allow me to introduce you to your new best friend.
AI medical scribing is the fastest way to cut down the documentation process.
They're exactly what they sound like: software designed to listen to patient encounters and write good clinical notes.
This isn't the only way teams are using AI. A recent survey found that nearly half of healthcare professionals using AI and automation in their practice saw a noticeable reduction in the time their staff spent on paperwork.
So how exactly does it work? AI in healthcare data management can be applied in various ways: from identifying outdated data to analyzing exam results.
But one of the simplest and most effective uses of AI is in clinical documentation.
How to use an AI scribe
- Press the recording button at the start of a patient visit, and Freed will take care of the rest.
- Press stop once you're done; Freed will complete your note in about a minute.
- Add in any edits, and Freed will learn to adapt to your style.
- Copy and paste your note to your EHR system.
Want to give it a try? Sign up for a free trial— no credit card required.
5. Mind basic legal considerations
Depending on your role, you might be one of the key players in keeping your practice compliant with privacy regulations at the local, state, and federal levels. Even if enforcing policies isn’t directly your responsibility, staying in the know about compliance requirements is crucial for protecting patient records and ensuring your daily operations run smoothly.
In the U.S., HIPAA is the star of the show when it comes to safeguarding patients' medical records and health information. This vital regulation ensures sensitive patient information stays confidential and secure, setting the gold standard for privacy in healthcare.
Staying HIPAA-compliant doesn’t have to feel overwhelming—just keep a few best practices in mind:
- Use secure, encrypted methods for sharing patient information electronically.
- Treat physical records with care by storing them securely and keeping them out of sight from unauthorized individuals.
- Limit access to patient information to only those who truly need it to do their jobs.
Don’t forget that state laws can add their own twists, particularly when it comes to how long patient records must be stored. HIPAA sets a baseline of six years, but local laws might extend that timeline to anywhere from six to ten years or more. Knowing the rules in your area is a must.
The good news? You can make life a lot easier by using tools that handle compliance for you. Whether you’re managing patient information with an electronic health records (EHR) system or other digital tools, look for platforms with strong encryption, secure access controls, and audit trails. These features not only protect patient records but also give you peace of mind knowing your EHR system has your back when it comes to compliance.
Note: All AI models used by Freed are HIPAA-compliant and don’t retain data. It deletes patient notes automatically once note summaries and quality checks are complete or within 30 days. You can also delete records manually at any time.
3 clinical note challenges & how to overcome them
In the spirit of SOAP, why don't dig into a good old problem list?
Here are the "chief complaints" (did I take the puns too far?) we've seen about writing clinical documentation, and how to solve them.
1. There's no time for clinical documentation
Sixty-four percent of healthcare professionals (that’s a whopping two-thirds!) feel overworked, juggling too many responsibilities during shifts.
Handling clinical notes only adds up to the many administrative tasks that make up your day.
With such a busy schedule, finding time to write detailed patient notes often means bringing work home (for some good old-fashioned pajama time).
Our goal is to find a way for healthcare providers to shut down their laptop after business hours.
💡 Clinical note solutions
If we can make the note-taking process take only 5-10 minutes, we can schedule short intervals throughout the day.
Here are some tips on how to write notes faster.
1. Use an AI Scribe— Tools like Freed will capture, transcribe, and write SOAP notes that you can easily copy/paste into your EHR.
“Goodbye to the avalanche of charts. I now leave at 5pm with all tasks done. Freed is a game changer. You can be up and running in minutes.” – Dr. Maryam Zarei, MD Allergy, Asthma, and Immunology, California
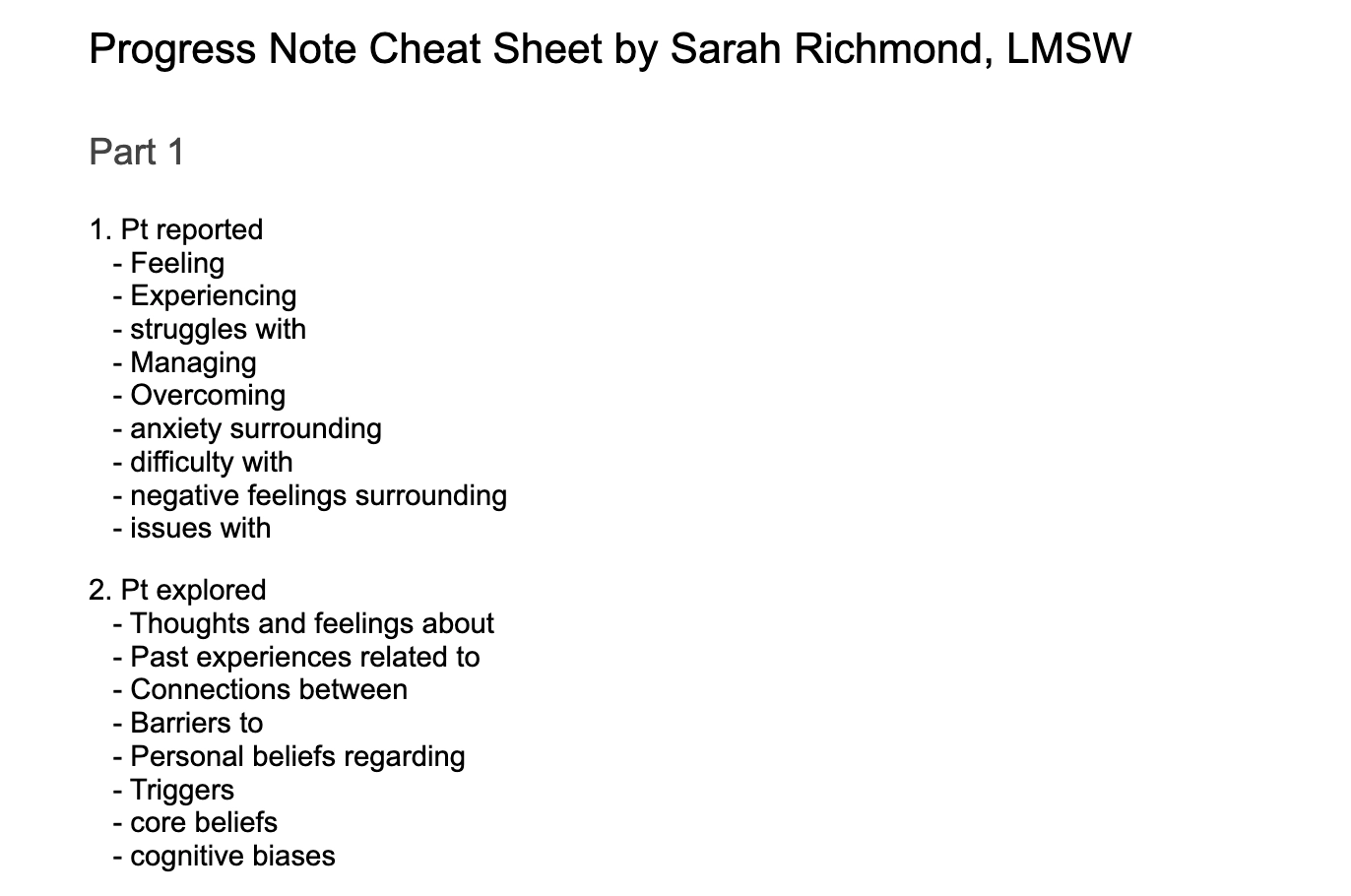
2. Use a cheatsheet—Write up a list of reported symptoms, explored causes, and identified symptoms that you can easily plug and play in your next visit.
Here's an example of a therapy note cheat sheet created by an LMSW.
3. Lean into shorthand and text shortcuts— Cut back on your words as much as possible by familiarizing yourself with abbreviations
“I make use of shorthand and common medical abbreviations. These cutbacks on words not only quicken the process of documentation but also ensure clarity in the notes.” — Dr. Sam Singh; Winit Clinic
You can take this a step further by leveraging technology. One clinician on reddit uses TextBlaze to auto-fill common terms and sentences into their note.

2. Avoiding note bloat
The "perfect" clinical note is concise, with just the right amount of detail.
It can be tough writing a comprehensive clinical note that's also clear and easy to read.
On top of that, different patients and situations require different levels of detail. For example, a past disease is only relevant in certain contexts— and that'll vary from case to case.
So, besides finding time to write your notes, you also need to be able to quickly sift through the information and filter out the most important points.
💡 Clinical note tips
Here are some practical ways to put only the most necessary information in your medical notes.
1. Take notes as soon as you can— If possible, schedule 10-15 minutes in between patient visits so that you can take notes ASAP. Now that you have tips on how to write notes faster, this next step helps you ensure accuracy and record retention.
“I try to document as close to the encounter as I can. That keeps the information fresh in my mind, so I miss fewer critical details and ensure that the information I put down is timely and accurate.” — Dr. Sham Singh, Winit Clinic
2. Find a format and stick to it— Whether you're opting for a traditional SOAP note or DAP structure, a standard template will help you organize your thoughts around the patient data you need.
2. Try a medical dictation or speech recognition tool—Take advantage of medical transcription AI to capture your conversations and observations in real time.
“To be able to dictate my notes and, further, have them typed out really enables me to take much more detailed observations at a speed so much faster than I could type. This helps me to record information in a much more natural flow since I can talk as I think.” — Dr. Sham Singh, Winit Clinic
3. Privacy concerns
Any data breach, whether accidental or not, can have serious consequences for both patients and healthcare providers.
To avoid it, you need to keep your notes compliant with basic legal considerations, privacy laws, and regulatory bodies (like HIPAA) in the U.S.
Of course, you don’t have to be an expert in information security or privacy laws.
Your organization should have clear policies in place for how to handle and store notes, and all you need is to stick to them. The tricky part is that with heavy workloads and tight schedules, even following established processes can be a challenge.
💡Clinical note solutions
1. Check your software for legal requirements— Ensure that all of your tools (including your medical note-taker or EHR) are HIPAA compliant and following industry best practices. This should be written in plain terms on any website.
2. Follow up with your clinic's legal requirements— Don't be afraid to check in with administrative team members in your healthcare organization if you're concerned about a process or tool. You and your patient's safety are worth it!
Benefits of better clinical documentation
Excellent clinical documentation does more than reduce headaches—it can make you happier (and healthier!) at your job and even improve patient outcomes.
Here are the biggest benefits of optimized clinical notes.
Happier clinicians
Seventy-seven percent of healthcare workers find themselves staying late at work because of too much documentation.
Imagine a weekend with 0 notes left. It might be closer than you think.
While we'll never eliminate the need for medical notes and data management in healthcare, you can definitely make the process more efficient and free up more of your time.
Consistent patient records
Once you master the balance between detail and structure, you'll find that documenting your clinical notes becomes way less of a slog: less time writing them and less time searching through them when patients come back.
Easier patient care coordination
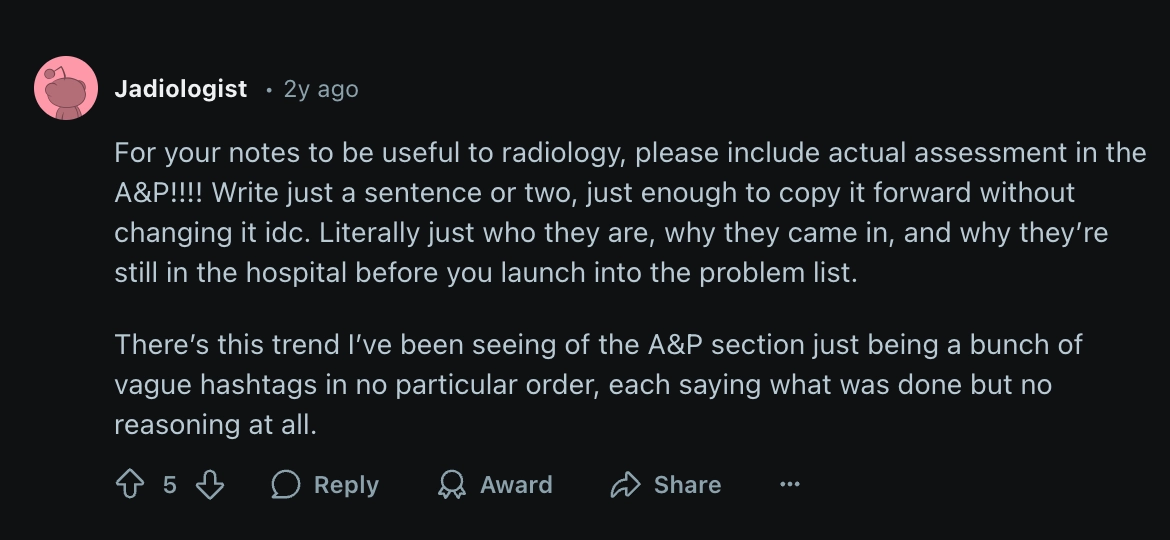
Clinical documentation passes through several hands— and everyone's looking for something different. The best thing we can do is make sure we're clear and pointed in our notes.
Higher-quality patient care
Paperwork takes time. And you don't have time to give.
Seven in ten clinicians say clinical documentation takes away from the time they’d rather spend with their patients.
When documentation starts to feel like a full-time job, it’s not just frustrating—it can impact the care you provide.
The good news? By streamlining your note-taking process, you can get that time back.
More accurate diagnoses
Good notes can help you catch symptoms and avoid any mix-ups with patient information—especially when diagnosing involves multiple exams and consultations.
When those exam results roll in, you’ll rely on your clinical notes to piece together an effective treatment plan. Clear and accurate notes not only guide your decisions but also help you minimize mistakes, ensuring top-notch patient care
Better legal protection
Detailed, accurate notes aren’t just good for patient care. They’re a safety net for you and your organization.
They provide a clear record of what happened, making it easier to navigate any legal issues that might arise.
By keeping your notes organized, you’ll always have solid documentation to back up your decisions and keep your practice running smoothly
Create excellent clinical documentation, fast
One final piece of advice: keep your clinical records standardized. No matter how busy you are or how simple the case appears, strive to include the same level of detail in every note.
Write your notes as if another practitioner will be taking over the patient's care—and they’ll always be clear and easy to understand.
Try Freed today and capture accurate clinical notes in seconds.
Table of Contents
Three things can be true:
- Clinical notes are the building blocks of any patient's medical record.
- With a good clinical note, we can easily monitor a patient's progress and outline a plan of care.
- They're also an overwhelming pain.
Let's face it: clinical documentation is no ones favorite part of the job. But they don't have to keep you up at night (literally).
There has to be a better way, and turns out: there is.
We've scoured forums and our personal network for tips from healthcare providers on how to:
- Quickly (and accurately) write clinical documentation;
- Avoid note bloat and prioritize important structured data;
- Ensure compliance in your medical records.
- Never take your notes home again.
Let's get started.
How to write clinical notes—a step-by-step guide
These notes are going down.
Here's a step-by-step guide on how to quickly write clinical notes while preserving key information.
1. Choose a framework or note template
First, you need to decide which format suits you best.
I'm sure your no stranger to the standard note templates:
- SOAP notes (or APSO)
- DAP notes
- BIRP notes
The choice really comes down to what you need to do with the information.
SOAP notes
SOAP (Subjective, Objective, Assessment, Plan) notes are a classic choice that works well for most clinical settings.
The four key components are:
- The patient’s report (Subjective);
- Your observations (Objective);
- Your evaluation (Assessment);
- The treatment plan (Plan).
It's a comprehensive clinical note type that's great for monitoring patient's progress and plan of care.
“I find that keeping the SOAP format-Subjective, Objective, Assessment, and Plan-keeps my notes organized and concise for other healthcare providers to more quickly comprehend the status and plan regarding the patient.” — Dr. Sham Singh, Winit Clinic
DAP notes
DAP notes (Data, Assessment, Plan) offer a more straightforward approach.
Unlike SOAP, which separates subjective and objective information, DAP notes combine both into a single section labeled "Data."
This patient data section provides a detailed description of the patient's symptoms and other relevant information.
BIRP notes
BIRP notes (Behavior, Intervention, Response, Plan) are best for mental health professionals.
They let you track:
- The patient’s behavior;
- What interventions you tried;
- How the patient responded;
- What’s next.
This framework helps capture detailed observations and responses, which is crucial for ongoing mental health care.
2. Make a list of must-have components
These frameworks are grate for structuring your notes. Now, we need to see what clinical information actually matters.
- Chief complaint: the main issue or reason the patient is seeking care.
- Review of systems (ROS): symptoms the patient is experiencing.
- Past medical history (PMH or Pmhx): Record any relevant past medical conditions, surgeries, or hospitalizations that could impact the current treatment.
- Medication history: list current medications, including dosages and any known allergies or adverse reactions. Tip: only focus on what's relevant.
- Physical examination findings: the results of your physical examination.
- Exam results: any lab results, imaging studies, or other diagnostic tests that were performed.
- Plan: further actions including the treatment plan, additional tests, and follow-up appointments.
💡 Tip: Focus on major findings and don't worry about copy/pasting every detail or full lab.
3. Lean on medical abbreviations
Is it a short cut or a lifeline?
Medical abbreviations in your notes will save you a lot of time.
Here are some abbreviations to get you to the finish line.
- BP — Blood Pressure
- HR — Heart Rate
- C/O — Complains Of
- WNL — Within Normal Limits
- Rx — Prescription
- H&P — History and Physical
- PMH — Past Medical History
- Dx — Diagnosis
It wouldn't hurt to look up some more medical abbreviations in medical textbooks or online medical dictionaries.
💡 Tip: There are online databases with comprehensive lists of standardized terminology and shorthands. Bookmark one for easy access.
4. Use an AI scribe
Allow me to introduce you to your new best friend.
AI medical scribing is the fastest way to cut down the documentation process.
They're exactly what they sound like: software designed to listen to patient encounters and write good clinical notes.
This isn't the only way teams are using AI. A recent survey found that nearly half of healthcare professionals using AI and automation in their practice saw a noticeable reduction in the time their staff spent on paperwork.
So how exactly does it work? AI in healthcare data management can be applied in various ways: from identifying outdated data to analyzing exam results.
But one of the simplest and most effective uses of AI is in clinical documentation.
How to use an AI scribe
- Press the recording button at the start of a patient visit, and Freed will take care of the rest.
- Press stop once you're done; Freed will complete your note in about a minute.
- Add in any edits, and Freed will learn to adapt to your style.
- Copy and paste your note to your EHR system.
Want to give it a try? Sign up for a free trial— no credit card required.
5. Mind basic legal considerations
Depending on your role, you might be one of the key players in keeping your practice compliant with privacy regulations at the local, state, and federal levels. Even if enforcing policies isn’t directly your responsibility, staying in the know about compliance requirements is crucial for protecting patient records and ensuring your daily operations run smoothly.
In the U.S., HIPAA is the star of the show when it comes to safeguarding patients' medical records and health information. This vital regulation ensures sensitive patient information stays confidential and secure, setting the gold standard for privacy in healthcare.
Staying HIPAA-compliant doesn’t have to feel overwhelming—just keep a few best practices in mind:
- Use secure, encrypted methods for sharing patient information electronically.
- Treat physical records with care by storing them securely and keeping them out of sight from unauthorized individuals.
- Limit access to patient information to only those who truly need it to do their jobs.
Don’t forget that state laws can add their own twists, particularly when it comes to how long patient records must be stored. HIPAA sets a baseline of six years, but local laws might extend that timeline to anywhere from six to ten years or more. Knowing the rules in your area is a must.
The good news? You can make life a lot easier by using tools that handle compliance for you. Whether you’re managing patient information with an electronic health records (EHR) system or other digital tools, look for platforms with strong encryption, secure access controls, and audit trails. These features not only protect patient records but also give you peace of mind knowing your EHR system has your back when it comes to compliance.
Note: All AI models used by Freed are HIPAA-compliant and don’t retain data. It deletes patient notes automatically once note summaries and quality checks are complete or within 30 days. You can also delete records manually at any time.
3 clinical note challenges & how to overcome them
In the spirit of SOAP, why don't dig into a good old problem list?
Here are the "chief complaints" (did I take the puns too far?) we've seen about writing clinical documentation, and how to solve them.
1. There's no time for clinical documentation
Sixty-four percent of healthcare professionals (that’s a whopping two-thirds!) feel overworked, juggling too many responsibilities during shifts.
Handling clinical notes only adds up to the many administrative tasks that make up your day.
With such a busy schedule, finding time to write detailed patient notes often means bringing work home (for some good old-fashioned pajama time).
Our goal is to find a way for healthcare providers to shut down their laptop after business hours.
💡 Clinical note solutions
If we can make the note-taking process take only 5-10 minutes, we can schedule short intervals throughout the day.
Here are some tips on how to write notes faster.
1. Use an AI Scribe— Tools like Freed will capture, transcribe, and write SOAP notes that you can easily copy/paste into your EHR.
“Goodbye to the avalanche of charts. I now leave at 5pm with all tasks done. Freed is a game changer. You can be up and running in minutes.” – Dr. Maryam Zarei, MD Allergy, Asthma, and Immunology, California
2. Use a cheatsheet—Write up a list of reported symptoms, explored causes, and identified symptoms that you can easily plug and play in your next visit.
Here's an example of a therapy note cheat sheet created by an LMSW.
3. Lean into shorthand and text shortcuts— Cut back on your words as much as possible by familiarizing yourself with abbreviations
“I make use of shorthand and common medical abbreviations. These cutbacks on words not only quicken the process of documentation but also ensure clarity in the notes.” — Dr. Sam Singh; Winit Clinic
You can take this a step further by leveraging technology. One clinician on reddit uses TextBlaze to auto-fill common terms and sentences into their note.
2. Avoiding note bloat
The "perfect" clinical note is concise, with just the right amount of detail.
It can be tough writing a comprehensive clinical note that's also clear and easy to read.
On top of that, different patients and situations require different levels of detail. For example, a past disease is only relevant in certain contexts— and that'll vary from case to case.
So, besides finding time to write your notes, you also need to be able to quickly sift through the information and filter out the most important points.
💡 Clinical note tips
Here are some practical ways to put only the most necessary information in your medical notes.
1. Take notes as soon as you can— If possible, schedule 10-15 minutes in between patient visits so that you can take notes ASAP. Now that you have tips on how to write notes faster, this next step helps you ensure accuracy and record retention.
“I try to document as close to the encounter as I can. That keeps the information fresh in my mind, so I miss fewer critical details and ensure that the information I put down is timely and accurate.” — Dr. Sham Singh, Winit Clinic
2. Find a format and stick to it— Whether you're opting for a traditional SOAP note or DAP structure, a standard template will help you organize your thoughts around the patient data you need.
2. Try a medical dictation or speech recognition tool—Take advantage of medical transcription AI to capture your conversations and observations in real time.
“To be able to dictate my notes and, further, have them typed out really enables me to take much more detailed observations at a speed so much faster than I could type. This helps me to record information in a much more natural flow since I can talk as I think.” — Dr. Sham Singh, Winit Clinic
3. Privacy concerns
Any data breach, whether accidental or not, can have serious consequences for both patients and healthcare providers.
To avoid it, you need to keep your notes compliant with basic legal considerations, privacy laws, and regulatory bodies (like HIPAA) in the U.S.
Of course, you don’t have to be an expert in information security or privacy laws.
Your organization should have clear policies in place for how to handle and store notes, and all you need is to stick to them. The tricky part is that with heavy workloads and tight schedules, even following established processes can be a challenge.
💡Clinical note solutions
1. Check your software for legal requirements— Ensure that all of your tools (including your medical note-taker or EHR) are HIPAA compliant and following industry best practices. This should be written in plain terms on any website.
2. Follow up with your clinic's legal requirements— Don't be afraid to check in with administrative team members in your healthcare organization if you're concerned about a process or tool. You and your patient's safety are worth it!
Benefits of better clinical documentation
Excellent clinical documentation does more than reduce headaches—it can make you happier (and healthier!) at your job and even improve patient outcomes.
Here are the biggest benefits of optimized clinical notes.
Happier clinicians
Seventy-seven percent of healthcare workers find themselves staying late at work because of too much documentation.
Imagine a weekend with 0 notes left. It might be closer than you think.
While we'll never eliminate the need for medical notes and data management in healthcare, you can definitely make the process more efficient and free up more of your time.
Consistent patient records
Once you master the balance between detail and structure, you'll find that documenting your clinical notes becomes way less of a slog: less time writing them and less time searching through them when patients come back.
Easier patient care coordination
Clinical documentation passes through several hands— and everyone's looking for something different. The best thing we can do is make sure we're clear and pointed in our notes.
Higher-quality patient care
Paperwork takes time. And you don't have time to give.
Seven in ten clinicians say clinical documentation takes away from the time they’d rather spend with their patients.
When documentation starts to feel like a full-time job, it’s not just frustrating—it can impact the care you provide.
The good news? By streamlining your note-taking process, you can get that time back.
More accurate diagnoses
Good notes can help you catch symptoms and avoid any mix-ups with patient information—especially when diagnosing involves multiple exams and consultations.
When those exam results roll in, you’ll rely on your clinical notes to piece together an effective treatment plan. Clear and accurate notes not only guide your decisions but also help you minimize mistakes, ensuring top-notch patient care
Better legal protection
Detailed, accurate notes aren’t just good for patient care. They’re a safety net for you and your organization.
They provide a clear record of what happened, making it easier to navigate any legal issues that might arise.
By keeping your notes organized, you’ll always have solid documentation to back up your decisions and keep your practice running smoothly
Create excellent clinical documentation, fast
One final piece of advice: keep your clinical records standardized. No matter how busy you are or how simple the case appears, strive to include the same level of detail in every note.
Write your notes as if another practitioner will be taking over the patient's care—and they’ll always be clear and easy to understand.
Try Freed today and capture accurate clinical notes in seconds.
FAQs
Frequently asked questions from clinicians and medical practitioners.
How should clinical notes be written?
What not to include in patient notes
How can I write clinical notes faster?
What is the AI app for clinical notes?

Related content
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.