Occupational therapy SOAP notes [+ Free Template]
Four sessions down. One kid nailed their fine motor goals, another melted down mid-dressing. And now, your next client’s waiting while your memory of the first session’s already fading.
SOAP notes should be your best friend — but right now they’re more like the coworker who keeps you late.
“SOAP notes can be tricky because we occupational therapists (OTs) are so detail-oriented,” said Janis Galindez, a registered occupational therapist.
But with a few solid tips and some practice, the SOAP notes that once took Galindez “forever” became no big deal.
In this guide: what a SOAP note actually looks like in occupational therapy practice, a simple template to start with, and a few tips Galindez swears by.
What is an occupational therapy SOAP Note?
SOAP notes are a staple in clinical documentation across healthcare.
For occupational therapists, they’re a necessity for documenting a plan of care and keeping tabs on everything that went into a therapeutic exercise.
Therapists are expected to record what occurs during sessions, reflect on client responses, and make clear recommendations for what comes next.
These notes hold weight for a supervising OTs, other care team members, school administrators, and insurance reviewers — almost like a cheat sheet for measuring a client’s progress
It’s not just paperwork — it’s your care plan in action.
In busy clinical settings, having this type of note capture a treatment plan helps therapists get clarity in their work, ensure quality of care, and clearly tcommunicate the value of interventions to the broader care team.
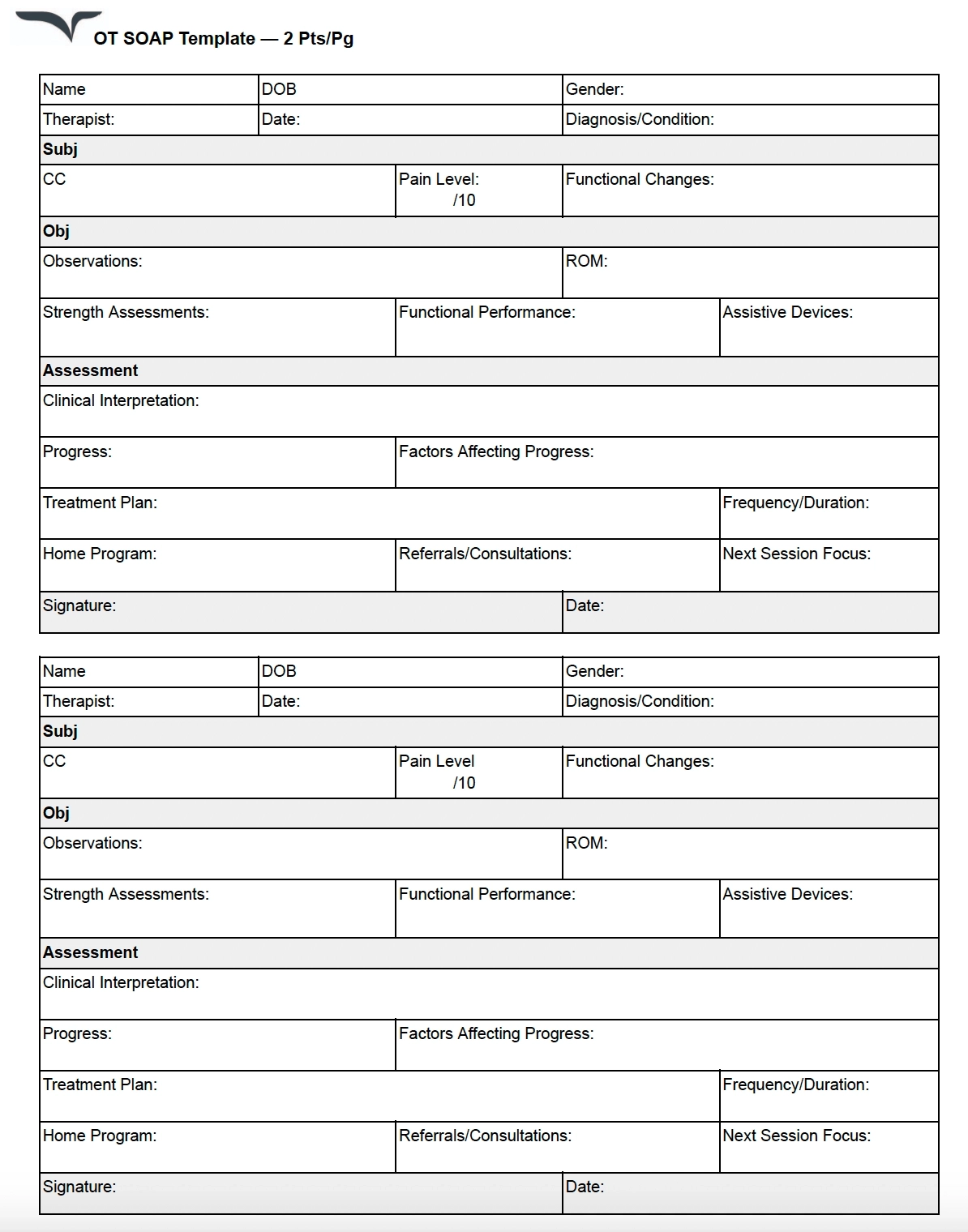
Free occupational therapy SOAP note template
Don’t want to start from scratch? Here’s a plug-and-play template to keep your notes focused and functional.
The SOAP note format for occupational therapy
SOAP stands for Subjective, Objective, Assessment, and Plan. Let’s break down what each section would look like if you’re an OT, occupational therapist assistant (OTA), or OT student.
Subjective
This section captures your client’s voice.
It can include your client’s (or their family and caregiver’s) own words about their current conditions — whether it’s physical discomfort, emotional barriers, or functional goals.
You might write:
- “Client reports left hand feels stiff in the morning and 'hurts when I try to hold my coffee mug.'”
- “Caregiver states client needed more help than usual during dressing this morning.”
Objective
Use this section to add more detailed observations and measurable data. This includes what the client did and how they did it.
Be specific, detailing factors like activity descriptions and client performance or participation.
You might write:
- “Client demonstrated improved pinch strength and good, sustained grip with right hand compared to last session.”
Assessment
In this assessment section, you’ll use your clinical reasoning to interpret the observations and data in the previous two sections.
You’ll want to explain what the data means, highlighting functional implications, barriers to progress, and the potential impact of continued therapy. This is a skilled judgment, not a summary.
You might write:
- “Client’s decreased grip strength continues to limit independence in ADLs and range of motion. Progress noted in tolerance to upper extremity exercises.”
Plan
The section is all about your next steps.
You can include what’s happening in the next session, what the client should do between sessions, recommendations for caregivers, or any specific follow-up actions.
You might write:
- “Continue current intervention plan focusing on fine motor tasks and ADL training. Introduce adaptive utensils next session. Educate caregiver on home exercise program.”
The benefits of SOAP notes for OTs
When done right, SOAP notes are more than just a documentation requirement. They keep OTs sane and ready to tackle a day of juggling multiple patient interactions while ensuring the best plan of care is documented with accuracy.
“As a pediatric OT you see so many clients and families, prepare for sessions, work on reports, and so much more that it is so easy to forget what you did with your kid in the last session,” says Galindez.
Here are a few reasons why Galindez uses the SOAP note as a preferred type of note:
- Jog your memory: When you’re juggling multiple clients and sessions, SOAP notes make it easier to recall what interventions you used and how a client responded, without relying on memory alone.
- Improve collaboration: Well-written notes help you communicate clearly with families, teachers, and other providers, keeping everyone on the same page about a client’s progress.
- Speed up with practice: Build your system, reuse smart blurbs, and suddenly notes aren’t the time suck they used to be.
Real-world examples of occupational therapy SOAP notes
Here’s a documentation example that illustrates how a SOAP note might look in different OT settings.
Example 1
Here’s a real-world SOAP note example shared on Reddit by an occupational therapist. This particular note captures a functional kitchen assessment with an adult patient.
Subjective: OT introduced self and explained the role. Verbal consent was obtained to complete a functional kitchen assessment.
Objective: Patient was seated upon arrival and performed an independent sit-to-stand transfer. Mobilized approximately 10 meters to the kitchen using a wheeled Zimmer frame (wzf). Initiated task by filling and plugging in the kettle. Located a mug, spoon, milk, and teabags with minimal supervision. Added the teabag to the mug, safely poured boiling water, added milk, and removed the teabag using the spoon. Patient then mobilized back to bedside with wzf.
Assessment: Patient demonstrated independent mobility with the use of a wzf and required no assistance with chair transfers. Successfully planned and sequenced the task of making a hot drink, indicating functional cognitive and physical abilities.
Plan: No further OT input required. Discharge from occupational therapy services.
Example 2
This second example is adapted from a school-based occupational therapy session featured on OT School House. It demonstrates how to document a handwriting-focused intervention with a student.
Subjective: The student reported having a rough day and mentioned hand fatigue from writing a three-page essay earlier.
Objective:
- Engaged in a 30-minute session focusing on handwriting and fine motor exercises.
- Demonstrated proper pencil grip in 80% of trials.
- Completed letter formation tasks with 90% accuracy.
Assessment: The student exhibits improved handwriting skills and endurance, but a limited range of motion. Hand fatigue appears related to extended writing tasks; however, overall performance indicates progress toward established goals.
Plan:
- Continue current handwriting intervention plan.
- Introduce strategies for managing hand fatigue during prolonged writing.
- Monitor and adjust the intervention plan as needed based on student feedback and performance.
The do’s and don’ts of effective occupational therapy SOAP notes
SOAP notes can save time (no, really).
Having good best practices and processes handy ensures that notetaking adds value and not unwanted effort into your workflow.
“I see about seven kids per day so writing SOAP notes can be overwhelming, especially when I am seeing kids back to back,” Galindez shares.
Here are a few more of her go-to strategies for managing SOAP notes without burning out:
- Take advantage of built-in breaks. If your schedule includes a few minutes after each session, use that time to jot down notes while the session is still fresh in your mind.
- Speak up about your workload. If you’re a student or new grad, don’t be afraid to advocate for protected documentation time. The goal you’re advocating is not just your ability to work properly, but it’s also about ensuring the best care for your clients.
- Explore in-session documentation (when appropriate). If it doesn’t interfere with your connection to the client, taking brief notes during a session can help reduce the backlog at the end of the day.
Here are some other tips to remember:
Do:
- Be detailed and concise. Focus on information that’s clinically relevant.
- Always relate your interventions back to function and occupation for the most effective therapy documentation.
- Keep your note purposeful and relevant to patient care by connecting activities to client goals during a particular occupational therapy session.
Don’t:
- Overwrite or include unnecessary descriptions that don’t impact care.
- Get lost in creative details without tying them to meaningful outcomes for an occupational therapy session.
- Assume a well-written note is a long note. Clarity is always the most important!
How to make SOAP notes work for you
Galindez’s biggest tip? Advocate for your time.
“I’m allotted a couple of minutes after each session for documentation at my current job, but I know this isn’t the case at every clinic,” she shares. “I always urge new students and new graduates to advocate for their time because having that is important for providing the best care.”
With a few smart tips, a reusable structure, and examples that speak your language, your notes can stop being the end-of-day headache — and actually help.
Want to skip the mental load and still get perfect notes? Try Freed's AI scribe.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing psychotherapy notes.
Table of Contents
Four sessions down. One kid nailed their fine motor goals, another melted down mid-dressing. And now, your next client’s waiting while your memory of the first session’s already fading.
SOAP notes should be your best friend — but right now they’re more like the coworker who keeps you late.
“SOAP notes can be tricky because we occupational therapists (OTs) are so detail-oriented,” said Janis Galindez, a registered occupational therapist.
But with a few solid tips and some practice, the SOAP notes that once took Galindez “forever” became no big deal.
In this guide: what a SOAP note actually looks like in occupational therapy practice, a simple template to start with, and a few tips Galindez swears by.
What is an occupational therapy SOAP Note?
SOAP notes are a staple in clinical documentation across healthcare.
For occupational therapists, they’re a necessity for documenting a plan of care and keeping tabs on everything that went into a therapeutic exercise.
Therapists are expected to record what occurs during sessions, reflect on client responses, and make clear recommendations for what comes next.
These notes hold weight for a supervising OTs, other care team members, school administrators, and insurance reviewers — almost like a cheat sheet for measuring a client’s progress
It’s not just paperwork — it’s your care plan in action.
In busy clinical settings, having this type of note capture a treatment plan helps therapists get clarity in their work, ensure quality of care, and clearly tcommunicate the value of interventions to the broader care team.
Free occupational therapy SOAP note template
Don’t want to start from scratch? Here’s a plug-and-play template to keep your notes focused and functional.
The SOAP note format for occupational therapy
SOAP stands for Subjective, Objective, Assessment, and Plan. Let’s break down what each section would look like if you’re an OT, occupational therapist assistant (OTA), or OT student.
Subjective
This section captures your client’s voice.
It can include your client’s (or their family and caregiver’s) own words about their current conditions — whether it’s physical discomfort, emotional barriers, or functional goals.
You might write:
- “Client reports left hand feels stiff in the morning and 'hurts when I try to hold my coffee mug.'”
- “Caregiver states client needed more help than usual during dressing this morning.”
Objective
Use this section to add more detailed observations and measurable data. This includes what the client did and how they did it.
Be specific, detailing factors like activity descriptions and client performance or participation.
You might write:
- “Client demonstrated improved pinch strength and good, sustained grip with right hand compared to last session.”
Assessment
In this assessment section, you’ll use your clinical reasoning to interpret the observations and data in the previous two sections.
You’ll want to explain what the data means, highlighting functional implications, barriers to progress, and the potential impact of continued therapy. This is a skilled judgment, not a summary.
You might write:
- “Client’s decreased grip strength continues to limit independence in ADLs and range of motion. Progress noted in tolerance to upper extremity exercises.”
Plan
The section is all about your next steps.
You can include what’s happening in the next session, what the client should do between sessions, recommendations for caregivers, or any specific follow-up actions.
You might write:
- “Continue current intervention plan focusing on fine motor tasks and ADL training. Introduce adaptive utensils next session. Educate caregiver on home exercise program.”
The benefits of SOAP notes for OTs
When done right, SOAP notes are more than just a documentation requirement. They keep OTs sane and ready to tackle a day of juggling multiple patient interactions while ensuring the best plan of care is documented with accuracy.
“As a pediatric OT you see so many clients and families, prepare for sessions, work on reports, and so much more that it is so easy to forget what you did with your kid in the last session,” says Galindez.
Here are a few reasons why Galindez uses the SOAP note as a preferred type of note:
- Jog your memory: When you’re juggling multiple clients and sessions, SOAP notes make it easier to recall what interventions you used and how a client responded, without relying on memory alone.
- Improve collaboration: Well-written notes help you communicate clearly with families, teachers, and other providers, keeping everyone on the same page about a client’s progress.
- Speed up with practice: Build your system, reuse smart blurbs, and suddenly notes aren’t the time suck they used to be.
Real-world examples of occupational therapy SOAP notes
Here’s a documentation example that illustrates how a SOAP note might look in different OT settings.
Example 1
Here’s a real-world SOAP note example shared on Reddit by an occupational therapist. This particular note captures a functional kitchen assessment with an adult patient.
Subjective: OT introduced self and explained the role. Verbal consent was obtained to complete a functional kitchen assessment.
Objective: Patient was seated upon arrival and performed an independent sit-to-stand transfer. Mobilized approximately 10 meters to the kitchen using a wheeled Zimmer frame (wzf). Initiated task by filling and plugging in the kettle. Located a mug, spoon, milk, and teabags with minimal supervision. Added the teabag to the mug, safely poured boiling water, added milk, and removed the teabag using the spoon. Patient then mobilized back to bedside with wzf.
Assessment: Patient demonstrated independent mobility with the use of a wzf and required no assistance with chair transfers. Successfully planned and sequenced the task of making a hot drink, indicating functional cognitive and physical abilities.
Plan: No further OT input required. Discharge from occupational therapy services.
Example 2
This second example is adapted from a school-based occupational therapy session featured on OT School House. It demonstrates how to document a handwriting-focused intervention with a student.
Subjective: The student reported having a rough day and mentioned hand fatigue from writing a three-page essay earlier.
Objective:
- Engaged in a 30-minute session focusing on handwriting and fine motor exercises.
- Demonstrated proper pencil grip in 80% of trials.
- Completed letter formation tasks with 90% accuracy.
Assessment: The student exhibits improved handwriting skills and endurance, but a limited range of motion. Hand fatigue appears related to extended writing tasks; however, overall performance indicates progress toward established goals.
Plan:
- Continue current handwriting intervention plan.
- Introduce strategies for managing hand fatigue during prolonged writing.
- Monitor and adjust the intervention plan as needed based on student feedback and performance.
The do’s and don’ts of effective occupational therapy SOAP notes
SOAP notes can save time (no, really).
Having good best practices and processes handy ensures that notetaking adds value and not unwanted effort into your workflow.
“I see about seven kids per day so writing SOAP notes can be overwhelming, especially when I am seeing kids back to back,” Galindez shares.
Here are a few more of her go-to strategies for managing SOAP notes without burning out:
- Take advantage of built-in breaks. If your schedule includes a few minutes after each session, use that time to jot down notes while the session is still fresh in your mind.
- Speak up about your workload. If you’re a student or new grad, don’t be afraid to advocate for protected documentation time. The goal you’re advocating is not just your ability to work properly, but it’s also about ensuring the best care for your clients.
- Explore in-session documentation (when appropriate). If it doesn’t interfere with your connection to the client, taking brief notes during a session can help reduce the backlog at the end of the day.
Here are some other tips to remember:
Do:
- Be detailed and concise. Focus on information that’s clinically relevant.
- Always relate your interventions back to function and occupation for the most effective therapy documentation.
- Keep your note purposeful and relevant to patient care by connecting activities to client goals during a particular occupational therapy session.
Don’t:
- Overwrite or include unnecessary descriptions that don’t impact care.
- Get lost in creative details without tying them to meaningful outcomes for an occupational therapy session.
- Assume a well-written note is a long note. Clarity is always the most important!
How to make SOAP notes work for you
Galindez’s biggest tip? Advocate for your time.
“I’m allotted a couple of minutes after each session for documentation at my current job, but I know this isn’t the case at every clinic,” she shares. “I always urge new students and new graduates to advocate for their time because having that is important for providing the best care.”
With a few smart tips, a reusable structure, and examples that speak your language, your notes can stop being the end-of-day headache — and actually help.
Want to skip the mental load and still get perfect notes? Try Freed's AI scribe.
Disclaimer: This article is for informational purposes only and does not constitute legal or clinical advice. Clinicians should follow applicable laws, regulations, and institutional policies when creating or sharing psychotherapy notes.
FAQs
Frequently asked questions from clinicians and medical practitioners.
What is an example of a SOAP note for OT?
What is the difference between an OT SOAP note and a discharge note?
How can I write an occupational therapy discharge note?
.avif)
Related content
.svg)
Free yourself for better things
548 Market Street, PMB 95301
San Francisco, CA 94104
Specialties
Compliance & Security
Our technology is HIPAA-compliant, uses industry best practices, and doesn’t store patient recordings.